")
American Journal of Gastroenterology ISSN 0002-9270
©_2006 by Am. Coll. of Gastroenterology doi: 10.1111/j.1572-0241.2006.00769.x
Published by Blackwell Publishing
Fasiha Kanwal, M.D., M.S.H.S.,1–4 Mary Farid, D.O.,1,3 Paul Martin, M.D.,6 Gary Chen, M.D.,6 Ian M. Gralnek, M.D., M.S.H.S.,2,3 Gareth S. Dulai, M.D., M.S.H.S.,2,3 and Brennan M. R. Spiegel, M.D., M.S.H.S.1–4
1Division of Gastroenterology, VA Greater Los Angeles Healthcare System, Los Angeles, California; 2Division of Digestive Diseases, David Geffen School of Medicine at UCLA, Los Angeles, California; 3UCLA/VA Center for Outcomes Research and Education (CORE), Los Angeles, California; 4CURE Digestive Diseases Research Center, Los Angeles, California; 5Mount Sinai School of Medicine, New York, New York; and 6Cedars Sinai Medical Center, Los Angeles, California
BACKGROUND:
Hepatitis B virus (HBV) patients with cirrhosis are at risk for developing costly, morbid, or mortal events, and therefore need highly effective therapies. Lamivudine is effective but is limited by viral resistance. In contrast, adefovir and entecavir have lower viral resistance, but are more expensive.
The most cost-effective approach is uncertain.
METHODS:
We evaluated the cost-effectiveness of six strategies in HBV cirrhosis: (1) No HBV treatment “do nothing”), (2) lamivudine monotherapy, (3) adefovir monotherapy, (4) lamivudine with crossover to adefovir on resistance (“adefovir salvage”), (5) entecavir monotherapy, or (6) lamivudine with crossover to entecavir on resistance (“entecavir salvage”). The primary outcome was the incremental cost per quality-adjusted life-year (QALY) gained.
RESULTS:
The “do nothing” strategy was least effective yet least expensive. Compared with “do nothing,” using adefovir cost an incremental $19,731. Entecavir was more effective yet more expensive than adefovir, and cost an incremental $25,626 per QALY gained versus adefovir. Selecting between entecavir versus adefovir was highly dependent on the third-party payer’s “willingess-to-pay” (e.g., 45% and 60% of patients fall within budget if willing-to-pay $10K and $50K per QALY gained for entecavir, respectively). Both lamivudine monotherapy and the “salvage” strategies were not cost-effective. However, between the two salvage strategies, “adefovir salvage” was more effective and less expensive than “entecavir salvage.”
CONCLUSION:
Both entecavir and adefovir are cost-effective in patients with HBV cirrhosis. Choosing between adefovir and entecavir is highly dependent on available budgets. In patients with HBV cirrhosis with previous lamivudine resistance, “adefovir salvage” appears more effective and less expensive than “entecavir salvage.”
(Am J Gastroenterol 2006;101:2076–2089)
BACKGROUND
Chronic hepatitisBvirus (HBV) infection is the leading cause of cirrhosis worldwide (1). The traditional cornerstone of treatment in HBV cirrhosis is lamivudine (2–4)—an agent favored because it is effective, easy to administer, and associated with few adverse effects (5–7). However, these benefits of lamivudine are counterbalanced by a high rate of viral resistance with prolonged therapy (8). Viral resistance has significant consequences in HBV patients with cirrhosis, because this subgroup is highly vulnerable with limited reserve of liver function (9, 10). Specifically, in comparison to HBV patients without cirrhosis, patients with cirrhosis are more likely to experience costly, morbid, or mortal events as a consequence of lamivudine resistance in comparison to HBV patients without cirrhosis (11).
Although we have previously shown that the new antiviral agents are unlikely to be cost-effective as initial therapy in HBV patients without cirrhosis (19), they may nonetheless have a health economic advantage in HBV patients with cirrhosis. This advantage not only arises because patients with HBV cirrhosis are at risk for developing resource intensive and life-threatening complications of liver disease, but also because they are more likely to develop these complications in the near term. Because health economic theory dictates that common and early events areweighted more heavily than late and rare events (20), the use of expensive yet effective therapies is likely to be more cost-effective in patients with cirrhosis than those with less advanced disease.
It is important to establish the most effective and costeffective therapeutic approach to HBV cirrhosis, especially in light of the increasing availability of new agents. Given the uncertainty regarding how best to use the available agents in this growing patient population, data from cost-effectiveness analyses may assist clinicians in everyday clinical decision making.We therefore performed an economic analysis to estimate the cost-effectiveness of competing strategies for the management of cirrhosis as a result of chronic HBV with active viral replication. We specifically sought to determine whether and under what circumstances the greater therapeutic benefits of newer antiviral agents, such as adefovir and entecavir, offset their greater cost versus lamivudine in the management of chronic hepatitis B cirrhosis.
METHODS
Decision Model Framework
MODEL OVERVIEW. Using decision analysis software (DATA 4.0, TreeAge Software, Inc.,Williamstown, MA), we evaluated a hypothetical cohort of 50-yr-old patients with chronic HBV cirrhosis and active viral replication. In order to emulate the case mix in clinical practice, we assumed that 50% of the cohort had compensated cirrhosis (i.e., Child’s Class A) and the remainder had decompensated cirrhosis (i.e., Child’s Class B or C).We subsequently varied the prevalence of decompensated cirrhosis between 0% and 100% in the sensitivity analysis, as described below. Patients entered the hypothetical model without previous treatment for HBV and received one of six competing strategies for the management of chronic HBV: (1) no pharmacological treatment of chronic HBV (“do nothing” strategy); (2) lamivudine monotherapy; (3) adefovir monotherapy; (4) lamivudine with crossover to adefovir on development of resistance (“adefovir salvage” strategy); (5) entecavir monotherapy; or (6) lamivudine with crossover to entecavir on development of resistance (“entecavir salvage” strategy).
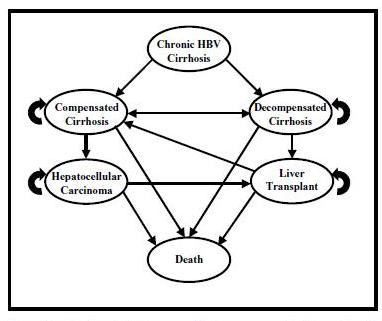
Figure 1. Markov state diagram. The base-case patient has chronic HBVinfection, clinical cirrhosis, active viral replication, and no previous treatment for hepatitis B. The clinician treats with one of four competing strategies: (1) “do nothing,” (2) lamivudine monotherapy, (3) adefovir monotherapy, and (4) “adefovir salvage” (see text for details). Within each strategy patients are stratified by stage of liver disease (i.e., compensated vs decompensated). During each 1-yr cycle individual patients either remain in their assigned health state (recursive arrow) or progress to a new health state (straight arrow). Transition rates between health states were derived from a systematic review of the literature (Tables 1 and 2). Refer to the Technical Appendix for additional information.
Because cirrhosis is a heterogeneous condition comprising patients with varying disease severity, we stratified our analysis by two groups: compensated versus decompensated cirrhosis. Furthermore, because the clinical course, outcomes, and resource usage vary in these two groups, we assigned separate probability estimates for compensated and decompensated cirrhosis (20–23). Patients entering the model either received no treatment (“do nothing”) or active treatment for chronic HBV, as described below. We then followed the co-hort over a lifetime horizon through a series of Markov cycles governing patient transitions between relevant health states (Fig. 1). Patients entered the model with either baseline compensated or decompensated cirrhosis. During each 1-yr cycle, individual patients either remained in their assigned health state (recursive arrow) or progressed to a new health state (straight arrow). Patients with compensated cirrhosis could develop decompensated cirrhosis (including variceal hemorrhage, ascites, or encephalopathy). In addition, patients with decompensated cirrhosiswere eligible to regress back to compensated cirrhosis (double-headed arrow). Following recompensation, patients were eligible to decompensate a second time. This rate of subsequent decompensationwas higher than the initial rate (not depicted in the model—see Appendix for details). Hepatocellular carcinoma could develop at any stage of cirrhosis. Patients with either decompensated cirrhosis or hepatocellular carcinoma were eligible to receive liver transplantation. Following liver transplantation, patients could develop recurrent HBV cirrhosis. These transition rates varied depending on both the treatment strategy employed and the presence or absence of underlying viral resistance (see Tables 1 and 2 and Appendix for details).
COMPETING STRATEGIES.
- “Do Nothing” Strategy: In this strategy, which served as the referent case for our analysis,we assumed that patients were followed clinically but did not receive pharmacological therapy for chronic hepatitisB. Patientswere subjected to the natural history of hepatitis B cirrhosis conditional on their stage of liver disease. We further assumed that all patients received regular ongoing care, including management of cirrhosis-related complications and hepatocellular carcinoma surveillance, as outlined by published management guidelines (2–4).We assumed that a proportion of patients with decompensation became eligible for liver transplantation, and further assumed that a subgroup of these patients subsequently received a liver transplantation at the rate reported by the United Network of Organ Sharing (49). We assumed that all transplanted patients received prophylaxis against recurrent hepatitis B with a combination of monthly hepatitis B immune globulin (HBIG) and daily lamivudine for an indefinite period, as recommended by current management guidelines (2–7).
-
Lamivudine Monotherapy Strategy: Patients in this strategy received up-front lamivudine 100mgorally once daily for an indefinite period, as recommended for cirrhosis by current management guidelines (2–4). Patients developing viral resistance continued receiving long-termlamivudine as recommended by published guidelines. Transplanted patients received prophylaxis with a combination of monthly HBIG and daily lamivudine for an indefinite period.
- Adefovir Monotherapy Strategy: Patients in this strategy received up-front adefovir 10 mg orally once daily for an indefinite period, as recommended for cirrhosis by current management guidelines (3, 4). Patients developing viral resistance continued receiving long-term adefovir. Transplanted patients received prophylaxis with a combination of monthly HBIG and daily adefovir for an indefinite period.
- Adefovir Salvage Strategy (Lamivudine to Adefovir Crossover): A relevant therapeutic alternative available to clinicians is a hybrid strategy of up-front lamivudine followed by “adefovir salvage” in case of developing lamivudine-related viral resistance. We assumed that patients in this strategy initially received lamivudine as described in the “lamivudine monotherapy strategy,” above. Patients were then crossed over to adefovir on developing viral resistance, and were subsequently managed as described in the “adefovir monotherapy strategy,” above. Patients without viral resistance remained on lamivudine. Therefore, adefovir was only reserved for patients developing viral resistance on lamivudine.
- Entecavir Monotherapy Strategy: Patients in this strategy received up-front adefovir 0.5 mg orally once daily for an indefinite period, as recommended for cirrhosis by current management guidelines (3, 4). Patients developing viral resistance continued receiving long-term adefovir. Transplanted patients received prophylaxis with a combination of monthly HBIG and daily adefovir for an indefinite period.
- Entecavir Salvage Strategy (Lamivudine to Entecavir Crossover): We assumed that patients in this strategy initially received lamivudine as described in the “lamivudine monotherapy strategy,” above. Patients were then crossed over to entecavir on developing viral resistance, and were subsequently managed as described in the “entecavir monotherapy strategy,” above. Patients without viral resistance remained on lamivudine. Therefore, entecavir was only reserved for patients developing viral resistance on lamivudine.
Clinical Probability Estimates
Our base-case model incorporated a wide range of estimates governing relevant clinical probabilities in the management and natural history of chronic hepatitis B cirrhosis (Tables 1 and 2). Our efficacy end points included clinical outcomes most relevant to patients with HBV cirrhosis, i.e., progression from compensated to decompensated cirrhosis, regression from decompensated to compensated cirrhosis, progression to hepatocellular cancer, progression to liver transplantation, and progression to cirrhosis and subsequent complications related to recurrent HBV postliver transplantation. We have used similar probability estimates in previous decision analysis in hepatitis B (19).We performed a systematic review of MEDLINE in order to derive these estimates. Refer to the Technical Appendix for a detailed description of our systematic review methodology.
Outcomes
Because the main objective of cost-effectiveness analysis is to permit comparisons between different interventions in medicine, and because quality-adjusted life-years (QALYs) are the exchange currency to allow for these comparisons to be made, we adopted QALYs as our main outcome (20). Our analysis reports the incremental cost per QALY gained between the competing strategies.
Utilities
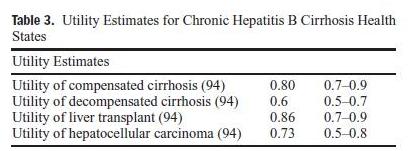
We incorporated a wide range of relevant health-state utilities in our model. Refer toTable 3 for the specific utility estimates, and to the Technical Appendix for a detailed description of these estimates.
Cost Estimates
We conducted our analysis from the perspective of a thirdparty payer and incorporated the direct health-care costs for a range of therapies, physician visits, diagnostic tests, and complications of chronic liver disease (Table 4).We obtained costs for physician services and procedures from the 2005 American Medical Association Current Procedural Terminology codebook and the 2005 Medicare Fee Schedule, and derived our base-case pharmaceutical costs from the average wholesale prices (AWPs) listed in the 2006 Red Book (16, 95). Because large buying consortiums are often capable of obtaining prices lower than the Red Book AWPs, we performed a sensitivity analysis using the acquisition costs of the Veteran’s Administration (VA) as a proxy for the discounts achieved by large third-party payers.We obtained cost estimates for cirrhosis and related health states from a published study of detailed itemized inpatient and outpatient direct costs incurred by patients with cirrhosis (96). As these costs were originally generated in 1997, we updated all the cost estimates to 2005 dollars using the medical care component of the consumer price index (97). We discounted all costs at a rate of 3% per yr (20).
Sensitivity Analyses
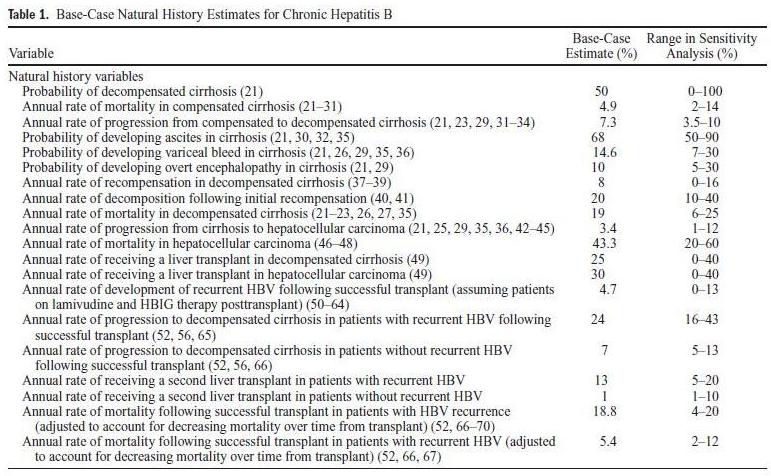
BASE-CASE SENSITIVITY ANALYSES. Table 1 lists our base-case probability estimates with the plausible range of values for each estimate. To test the influence of all variables on the model results, we performed a multivariable sensitivity analysis (“tornado analysis”) and rank-ordered the most influential variables (98).We then performed one-way sensitivity analyses on the most influential variables.
Whereas one-way sensitivity analyses provide information regarding the robustness of a model, they are inadequate to simulate real-world conditions. To acknowledge the reality that each individual carries a unique composition of clinical probabilities, we conducted a probabilistic (Monte Carlo) simulation under the assumption that all variables were triangular in distribution (98). The triangular distribution assumes that a parameter’s base-case value is most likely to occur and that the minimum and maximum values are least likely to occur. The probability of observing a value between the basecase and extreme value is linearly interpolated.We simulated 2,000 trials and plotted the results on cost-effectiveness acceptability curves stratified by willingness-to-pay thresholds (99). We analyzed the base-case cohort to find the 2.5th and 97.5th percentiles for our estimate of incremental cost per QALY gained among competing strategies.
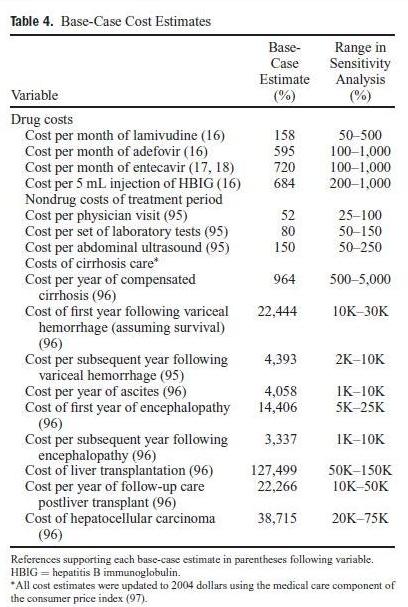
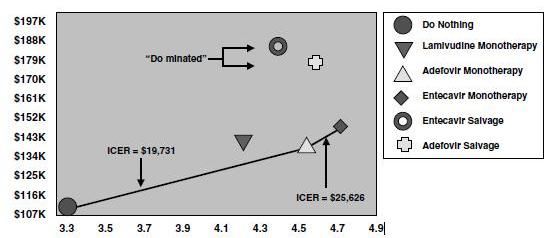
Figure 2. Base-case cost-utility results. The base-case analysis assumes that half of the patients have decompensated cirrhosis and half have compensated cirrhosis. The vertical axis below displays the lifetime cumulative cost, and the horizontal axis displays the QALYs gained. The “do nothing” strategy is located at the origin and is the least effective yet least expensive of the six competing strategies. Each diagonal line represents the incremental cost-effectiveness ratio (ICER) between the connected strategies. The ICER between strategies represents the additional cost that must be expended to gain one additional QALY when adopting the more expensive of the two compared strategies. For example, the use of etecavir monotherapy instead of adefovir monotherapy cost an additional $26,626 to gain one additional QALY. The “adefovir salvage,” “entecavir salvage,” and lamivudine monotherapy strategies are “dominated” (i.e., more expensive yet less effective than alternatives) because they fall above and to the left of the border that outlines the other three strategies that compose the “cost-effectiveness frontier.”
RESULTS
Base-Case Results
The results of our base-case analysis are displayed in Figure 2. The “do nothing” strategy was the least expensive yet least effective of the four competing strategies. Compared with doing nothing, using adefovir monotherapy cost an incremental $19,731 to gain one additional QALY (2.5th and 97.5th percentiles, $14,342 and $24,224). Compared with adefovir, entecavir monotherapy cost an incremental $25,626 per QALY-gained (2.5th and 97.5th percentiles, $19,637 and $31,184). Therefore, entecavir monotherapy was more effective yet more expensive than adefovir monotherapy. Both the lamivudine monotherapy and “salvage” strategies (i.e., “adefovir salvage” and “entecavir salvage”) were more expensive yet less effective than competing strategies, and were therefore “dominated,” suggesting that initial therapy with lowresistance therapies (e.g., adefovir or entecavir) is more costeffective than reserving these therapies for the development of lamivudine resistance.
Base-Case Sensitivity Analyses
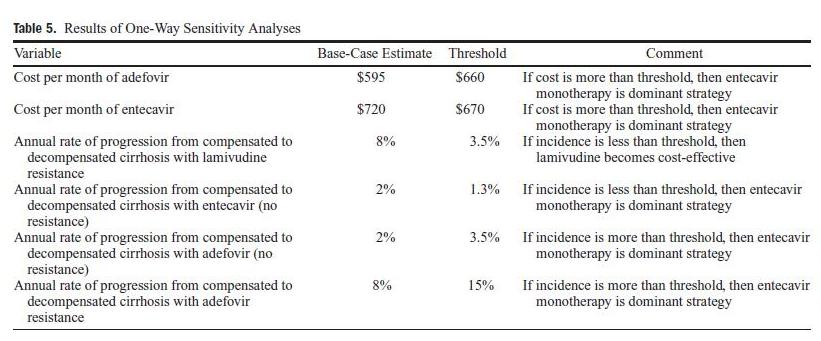
Tornado analysis revealed that the model was sensitive to six variables. Table 5 displays the results of one-way sensitivity analyses for these variables in decreasing order of influence, and lists the thresholds in which the cost-effectiveness order between the strategies changed. The remaining variables did not impact the model when varied over a wide range. In particular, the results were qualitatively similar regardless of the ratio of patients with compensated versus decompensated cirrhosis. Similarly, the results of our sensitivity analysis employing VA acquisition costs for pharmaceuticals were qualitatively similar to our base-case results (results not shown).
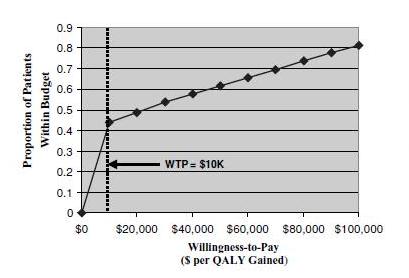
Our results suggest that of the five active therapeutic strategies, both the entecavir and adefovir monotherapy strategies were potentially cost-effective. To help determine whether to use adefovir or entecavir under different budgetary restraints, we performed a Monte Carlo analysis with 2,000 simulations to compare entecavir and adefovir monotherapy across a range of willingness-to-pay thresholds (Fig. 3). The analysis revealed that the decision to pay more money for better effectiveness depended highly on the available budget. For example, if a third-party payer was only willing to spend an additional $10,000 per QALY gained for entecavir, then 45% of patients would fall within the budget. In contrast, if a third-party payer was willing to pay $50,000 per QALY gained, then 60% of patients would fall within the budget.
DISCUSSION
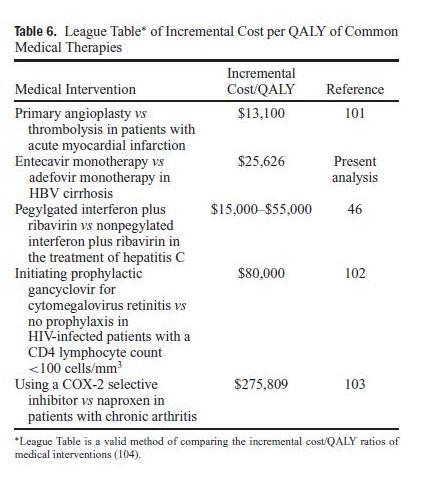
The most cost-effective strategy in the management of HBV cirrhosis remains unclear.We performed a comprehensive decision analysis to identify the most cost-effective therapeutic approach under varying clinical and budgetary conditions. Our analysis has four key findings. First, we found that the newer generation of antiviral therapies inHBV, including adefovir and entecavir, are cost-effective in patients with HBV cirrhosis and should be preferred over lamivudine monotherapy. Second, of the competing new-generation antiviral therapies, entecavir appears to be more effective yet more expensive than adefovir. Specifically, compared with adefovir, treating with up-front entecavir cost an additional $25,626 to gain one additional QALY—a value that falls well within the range of many commonly accepted medical interventions (Table 6). Third, selecting between adefovir and entecavir is highly dependent on available budgets and “willingness to pay” (Fig. 3). For third-party payers willing to pay $50,000 perQALYgained for entecavir, most (>60%) patients receiving entecavir will fall within the budget. In contrast, entecavir is generally not cost-effective for third-party payers willing to pay less than $25,000 per QALY gained. Fourth, our analysis found that initiating up-front lamivudine with crossover to adefovir or entecavir as “salvage” on emergence of viral resistance is not cost-effective in HBV patients with cirrhosis. However, when faced with a patient who has already developed lamivudine resistance, using “adefovir salvage” appears more effective and less expensive than “entecavir salvage” on the basis of current viral resistance data (12, 100, 109).
These results are consistent with our a priori hypothesis that expensive yet effective therapies are more cost-effective in patients with cirrhosis than those without cirrhosis. This hypothesis is supported by the health economic theory that early and frequent events are weighted more heavily than late and rare events (20). In the case of cirrhosis—a health state plagued by the specter of impending clinical complications— patients may develop resource-intensive, morbid, or mortal complications in short order. In contrast, most HBV patients without cirrhosis either never develop complications of chronic liver disease or else develop complications after a 10–20-yr lead period. Although antiviral resistance is never a goal of therapy in either group of patients, the development of resistance has less severe health economic consequences in noncirrhotics than cirrhotics, because patients with cirrhosis can ill afford the emergence of viral resistance and subsequent viral flares (11). Taken together, these factors strengthen the argument for employing effective therapies in cirrhosis, not only to improve effectiveness, but also to improve cost-effectiveness.
This analysis has several strengths. First, this is the only study to date that compares all of the currently approved agents for chronic HBV cirrhosis, and in particular incorporates the most recent data for entecavir. In light of the increasing availability of newer agents, coupled with the attendant uncertainty regarding how best to select between these agents, our model helps to direct clinical decision making in a cost-conscious environment. Second, our model acknowledges the heterogeneity in liver disease severity seen in clinical practice. Specifically, we stratified our analyses by the stage of liver disease, and accounted for the variations in clinical course, prognosis, and response to therapy between patients with compensated versus decompensated cirrhosis. This approach increases the generalizability of our findings. Third, our model attempts to reflect the everyday challenges in the management of patients with HBV cirrhosis. For example, we account for noncompliance with medical therapy, noncompliance with physician follow-up visits, renal side effects of adefovir, development of clinical recompensation in patients with initially decompensated cirrhosis, development of second decompensation among patients with previous recompensation, poor availability of donor organs for eligible patients, immune prophylaxis after liver transplantation, and HBVrecurrence following liver transplantation. By acknowledging these practical issues, our analysis is more likely to reflect the health economic consequences of everyday practice.
There are several limitations to our analysis. First, several of our estimates are derived from studies of varying design, patient population, follow-up time, and quality. However, we have attempted to guard against inaccurate base-case results by systematically reviewing the literature, calculating weighted means to account for study sample size, and relying on preexisting meta-analyses when available. Second, our estimates of patient health preferences may be limited because we adopted utilities for cirrhosis and related complications resulting from hepatitis C, not HBV. However, it is reasonable to assume that a patient developing cirrhosis or related complications should suffer similar quality-of-life decrement regardless of whether their cirrhosis resulted from hepatitis B or hepatitis C. Moreover, our results did not change despite varying our utility estimates over a wide range in multiple forms of sensitivity analysis. Third, we did not evaluate the potential strategy of up-front treatment with interferon. Although this approach is a relevant strategy in patients with histological cirrhosis, its role in clinically significant cirrhosis has been limited given the risk of causing (sometimes fatal) disease flare-ups (11). Because practice guidelines recommend against the use of interferon in patients with clinical cirrhosis (3, 4), we did not model interferon monotherapy in this analysis. Last, our analysis only applies to a narrow patient population. Specifically, our hypothetical cohort has HBV-related clinical cirrhosis, evidence of viral replication, and no contraindications to therapy. Therefore, our results may not be applicable to alternative populations, including those without viral replication, those with histological (but not clinical) cirrhosis, and postliver transplantation.However, because our base-case cohort reflects the most common and clinically relevant presentation of patients with HBV cirrhosis, we believe our data are applicable to most patients with HBV cirrhosis, and are especially relevant to the communitybased practice settings.
In conclusion, our analysis reveals that both adefovir and entacavir are cost-effective in the management of HBV cirrhosis, and these agents should be preferred over lamivudine as first-line therapy in this vulnerable subgroup of patients. Selecting between adefovir and entecavir is highly dependent on budgetary restraints and willingness to pay. Among patients with HBV cirrhosis who have previously developed lamivudine resistance, “adefovir salvage” appears more cost-effective than “entacavir salvage.” As our knowledge about resistance patterns of these agents becomes better refined with longer term follow-up, these cost-effectiveness data may ultimately change with time. Therefore, future research should aim to prospectively measure the accrued cost and effectiveness of these competing management strategies in patients with HBV cirrhosis, and should specifically measure the impact of viral resistance patterns on health economic outcomes.
TECHNICAL APPENDIX
Systematic Review Methodology
We conducted a structured search of MEDLINE to identify relevant English language studies from January 1970 to March 2006. In addition, we reviewed the bibliographies of key review articles for references not captured by our search strategy. We targeted studies that address either the natural history of HBV cirrhosis, including the posttransplantation course, or the efficacy of lamivudine, adefovir, or entecavir in the treatment of both pre- and posttransplantation HBV. The keywords and search strings used to perform the systematic review are available from the authors on request.
Three reviewers (FK, MF, BS) assessed the generated titles for relevancy and only rejected titles that fulfilled the following explicit exclusion criteria: (1) not written in English, (2) not concerning human subjects, (3) not related to
chronic viral hepatitis, and (4) solely related to cholestatic liver diseases, autoimmune liver diseases, or metabolic liver diseases. The reviewers then individually assessed the relevancy of all abstracts corresponding to the remaining titles and excluded abstracts for the following reasons: (1) fulfilled one or more of the title exclusion criteria, (2) did not pertain to one or more of the following estimates: progression rate to decompensated cirrhosis, progression rate to hepatocellular carcinoma, health state-specific mortality rate, progression rate to recompensated cirrhosis, annual rate of viral resistance on therapy, or posttransplantation recurrence of HBV and subsequent consequences, and (3) were solely limited to the pediatric population. The reviewers then assessed the relevancy of all manuscripts corresponding to the remaining abstracts, and included manuscripts if they had data pertaining to the probability estimates required for the model (Tables 1 and 2). Where available, we relied on summary estimates derived from published systematic reviews and meta-analyses.
For each study, we converted all available data into annual probability estimates for use in the Markov model. We calculated these annual estimates using the standard transformation formula p = 1 − e−rt, where p is the probability, e is the base of the natural logarithm, r is the event rate, and t is the time interval (105).We then combined all the data across studies by calculating a weighted mean using study sample size as the weight. We also recorded the range of values reported in the literature, and conducted sensitivity analyses to span this range. Each estimate reported in Tables 1 and 2 (and discussed below) represents the weighted mean for the corresponding probability estimate.
Systematic Review Results
The search strategy identified 4,771 titles, of which 192 met our explicit inclusion criteria. Of these, 91 addressed natural history estimates, 83 addressed efficacy of the antiviral agents in pretransplant HBV (50 addressed lamivudine efficacy estimates, 20 addressed adefovir efficacy estimates, 8 addressed entecavir efficacy estimates), and 23 addressed efficacy of the antiviral agents in posttransplant HBV.
NATURAL HISTORY ESTIMATES
- Progression to Decompensated Cirrhosis: Our analysis found an annual rate of progression from compensated to decompensated cirrhosis inHBVof 7.3% (range 3.4–10% per yr) (21, 23, 29, 31–34). Among those patients with decompensated cirrhosis, the probability of developing ascites, variceal hemorrhage, and overt encephalopathy was 68% (21, 30, 32, 35), 14.6% (21, 26, 29, 35, 36), and 10% (21, 29), respectively. The annual mortality rates in compensated and decompensated cirrhosis were 4.9% (21–31) and 19% (21–23, 26, 27, 35), respectively.
- Regression from Decompensated to Compensated Cirrhosis: Our review found that 8% of patients with decompensated cirrhosis regressed back to compensated cirrhosis, i.e., recompensated (range 0–16%) (37–39). In our model, we assumed that these recompensated patients could then decompensate for the second time.
- Progression to Hepatocellular Carcinoma: Patients with HBV cirrhosis developed hepatocellular carcinoma at a rate of 3.4% per yr (range 0.8–12% per yr) (21, 25, 29, 35, 36, 42–45). The annual mortality rate in hepatocellular carcinoma was 43.3% (46–48).
- Progression to Cirrhosis and Subsequent Complications with Recurrent HBV: We assumed that all patients received prophylaxis against recurrent HBV (see “Methods” section).We found that only 4.7% of patients receiving a combination of HBIG and lamivudine developed recurrent HBV per yr (range 0–13%) (50–64).We did not find any studies reporting the HBV recurrence rate in patients receiving prophylaxis with a combination of HBIG and adefovir. In the absence of data, we assumed that the rate of HBV recurrence was the same between protocols using lamivudine and adefovir, and therefore set the rate for HBIG and adefovir at 4.7% per yr.
Treatment Efficacy Estimates
-
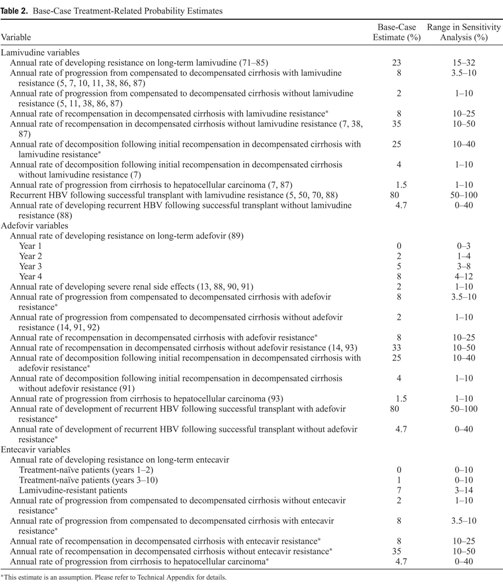
Lamivudine Efficacy Estimates: Our review indicated that 23% of patients developed viral resistance annually (i.e., development of YMDD mutation) on lamivudine therapy (71–85). In our model, the disease progression rates and response to treatment differ between those with and without viral resistance. Our review showed that 2% of cirrhotic patients without viral resistance who were maintained on long-term lamivudine developed decompensation annually (5, 11, 38, 86, 87) versus 8% of patients with viral resistance (5, 7, 10, 11, 38, 86, 87). We found that 35% of patients with decompensated cirrhosis (i.e., Child class B or C) without viral resistance regressed to compensated cirrhosis (i.e., Child class A) (7, 38, 87), and that only a few patients developed second decompensation on long-term therapy (7). We did not find data regarding the rate of regression from decompensated to compensated cirrhosis in patients with viral resistance on long-term lamivudine. In the absence of data, we adopted the rate of 8% per yr observed in natural history studies.
- Adefovir Efficacy Estimates:We found several studies that report data on the efficacy of adefovir among cirrhotic patients with preexisting lamivudine resistance (i.e., “adefovir salvage” strategy). However,we did not find any data on the efficacy of adefovir monotherapy among treatmentna ¨ıve patients with cirrhosis. In the absence of these data, we assumed that the efficacy of adefovir among cirrhotics was the same regardless ofwhether or not patients had previously developed lamivudine resistance. This assumption has face validity because the annual rate of durable virologic response on adefovir is the same independent of previous lamivudine resistance (106–108). Our review found that the annual rate of viral resistance during year 1, 2, 3, and 4 was 0%, 2%, 5%, and 8%, respectively (with a cumulative rate of 18% over 4 yr) (89).We found that 2% of cirrhotic patients developed decompensation annually (14, 91, 92), and that 33% of patients with decompensated cirrhosis regressed to compensated cirrhosis annually in the absence of viral resistance on long-term adefovir (14, 93). Our review did not find data on the rates of disease progression and regression in patients with adefovir resistance. We therefore assumed that these rates were similar to the corresponding estimates in patients with viral resistance on long-term lamivudine.
- Entecavir Efficacy Estimates: There are no long-termdata currently available regarding the clinical efficacy or antiviral resistance patterns of entecavir. In the absence of entecavir data regarding our efficacy end points (i.e., clinical outcomes most relevant to patients with HBV cirrhosis including progression to decompensated cirrhosis, regression from decompensated to compensated cirrhosis, progression to hepatocellular cancer, or progression to liver transplantation)we relied on histological improvement as the best surrogate of improved long-term clinical outcomes. Our analysis stratifies patients into those with versus without viral resistance, and uses separate clinical efficacy estimates for both strata. Using this approach, our review revealed that, as compared with adefovir and entecavir, lamivudine use is associated with the highest rate of histological improvement. There are no peer-reviewed data available on the rate of fibrosis reduction with entecavir use. The data for the adefovir and lamivudine showthat, as compared with adefovir, lamivudine use resulted in a greater reduction in the fibrosis scores among patients without evidence of viral resistance. In a recent independent systematic review, Dienstag et al. found no differences in the degree of histological improvements (including both necroinflammation and fibrosis score improvements) among studies reporting entecavir and lamivudine use in HBV, even after adjusting for lamivudine resistance (15). Based on these data, we assumed that entecavir had equal efficacy to lamivudine (12, 110–114). Short-term data indicate that the annual incidence of viral resistance with entecavir is 0% in treatment-na¨ıve patients (12, 109), and7%in patients with previous lamivudine resistance (100), and we used these estimates for the entecavir monotherapy and “entecavir salvage” strategy, respectively. Specifically, we assumed that there was no viral resistance from entecavir during the first 2 yr of therapy. Furthermore, we assumed that the rate of subsequent viral resistance with entecavir remained minimal, and never exceeded 1% over the entire course of therapy—an assumption that likely underestimates what will happen as longer term data are collected with entecavir (based on the experience of other antiviral agents, which are uniformly associated with increasing resistance over time).
- Progression to Cirrhosis and Subsequent Complications with Recurrent HBV: We assumed that all patients received prophylaxis against recurrent HBV following liver transplantation (see “Methods” section). We further assumed that the rates of recurrent HBV varied depending on the presence or absence of pretransplant viral resistance. We found that less than 5% of patients without pretransplant viral resistance who subsequently received posttransplant HBIG and lamivudine developed recurrent HBV per yr (range 0–13%) (88). We did not find any studies that report the rate of HBV recurrence in patients receiving prophylaxis with a combination of HBIG and adefovir. In the absence of data, we assumed that the rate of HBV recurrence was the same between protocols using lamivudine and adefovir, and therefore set the rate for HBIG and adefovir at 4.7% per yr. We assumed that 80% of patients with pretransplant viral resistance subsequently developed HBV recurrence posttransplant if continued on the same agent post-OLT (5, 50, 70, 88). In contrast to the patients in the lamivudine or adefovir monotherapy strategy, those in the “adefovir salvage” strategy (i.e., patients with lamivudine resistance who cross over to adefovir pre-OLT) developed recurrent HBV at low rates. In a recent study, Marzano et al. reported that none of their 11 patients who were started on adefovir on development of lamivudine resistance experienced viral recurrence during the 3-yr study follow-up (88). Because the rate reported by Marzano et al. may underrepresent the true HBV recurrence rate because of the small number of patients, we set the corresponding rate to 4.7%—rate adopted for HBV recurrence without pre-OLT viral resistance (see above). Our review found that 24% of patients with recurrent HBV following liver transplantation developed graft failure per yr (range 16–43%) (52, 56, 65). In contrast, only 7%of patients without recurrent HBV developed graft failure per yr (range 5– 13%) (52, 56, 66). The annual mortality rates in patients with and without recurrent HBV were 18.8% (52, 66–70) and 5.4% (52, 66, 67), respectively.
Utility Estimates
Patients with chronic viral hepatitis experience a wide range of health states that may diminish their health-related quality of life. Several studies in hepatitis C have measured patient health preferences, or utilities, for complications of chronic liver disease, including compensated cirrhosis, decompensated cirrhosis, hepatocellular carcinoma, and liver transplantation (94, 115). There are no similar studies in HBV. However, both hepatitis C and HBV lead to cirrhosis and related complications, and there is no a priori reason to believe that the quality-of-life decrement engendered by these health states would vary by underlying etiology. In other words, cirrhosis is the end result of a common pathway shared by both forms of viral hepatitis, and a patient developing cirrhosis should suffer the same quality-of-life decrement independent of the etiology of cirrhosis in the first place. We therefore adopted previously established utilities for cirrhosis and related complications that were derived using standard gamble elicitations in patients with chronic hepatitis C (94). Specifically, we assumed a utility of 0.82 for compensated cirrhosis, 0.60 for decompensated cirrhosis, 0.86 following successful liver transplant, and 0.73 for hepatocellular carcinoma (94). Because our base-case utility estimates are unlikely to be precisely reproduced in varying populations, we varied each estimate over a wide range in sensitivity analysis as described below. Table 3 provides the full list of utilities and the range tested in sensitivity analysis around each point estimate. We discounted all utilities at a rate of 3% per yr as recommended by the National Panel on Cost-Effectiveness in Health and Medicine (20).
STUDY HIGHLIGHTS
What Is Current Knowledge
- It is controversial whether the improved efficacy of the new-generation antiviral agents for hepatitis B, including adefovir and entecavir, offsets the cost versus lamivudine for the management of hepatitis B patients with cirrhosis.
What Is New Here
- Both adefovir and entecavir seem to be cost-effective in hepatitis B patients with cirrhosis.
- Of the new agents, entecavir appears more effective yet more expensive than adefovir. Selecting between these agents completely depends upon the available health care budget and willingness-to pay.
- In patients with pre-existing lamivudine resistance, it appears more cost-effective to start with adefovir than entecavir, since entecavir is associated with higher viral resistance than adefovir in the face of previous lamivudine resistance.
REFERENCES
- Cirrhosis of the liver. National Institute of Digestive and Diabetes and Kidney Diseases. Available at: http://www.digestive.niddk.nih.gov/ddiseases/pubs/cirrhosis/ (Accessed).
- Lok ASF, McMohen B. Chronic hepatitis B. Hepatology 2001;34:1225–41.
- Fung SK, Lok AS. Management of patients with hepatitis B virus-induced cirrhosis. J Hepatol 2005;42:S54–64.
- Keeffe EB, Dieterich DT, Han SH, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States. Clin Gastroenterol Hepatol 2004;2:87–106.
- Perrillo RP, Wright T, Rakela J, et al. A multicenter United States-Canadian trial to assess lamivudine Monotherapy before and after liver transplantation for chronic hepatitis B. Hepatology 2001;33:424–32.
- Villeneuve JP, Condreay LD, Willems B, et al. Lamivudine treatment for decompensated cirrhosis resulting from chronic hepatitis B. Hepatology 2000;31:207–10.
- Yao FY, Bass NM. Lamivudine treatment in patients with severely decompensated cirrhosis due to replicating hepatitis B infection. J Hepatol 2000;33:301–7.
- Atkins M, Hunt CM, Brown N, et al. Clinical significance of YMDD mutant hepatitis B virus in a large cohort of lamivudine-treated hepatitis B patients (abstract). Hepatology 1998;28:319A.
- de Man RA, Bartholomeusz A, Niesters HGM, et al. The sequential occurrence of viral mutations in a liver transplant recipient re-infected with hepatitis B: Hepatitis B immune globulin escape, famciclovir non-response, followed by lamivudine resistance resulting in graft loss. J Hepatol 1998;29:669–75.
- Fontana RJ, Hann HW, Perrillo RP, et al. Determinants of early mortality in patients with decompensated chronic hepatitis B treated with antiviral therapy. Gastroenterology 2002;123:719–27.
- DiMarco VD, Marzano A, Lampertico P, et al. Clinical outcome of HBeAg-negative chronic hepatitis B in relation to virological response to lamivudine. Hepatology 2004;40:883–91.
- Lai CL, Rosmawati M, Lao J, et al. Entecavir is superior to lamivudine in reducing hepatitis B virus DNA in patients with chronic hepatitis B infection. Gastroenterology 2002;123:1831–8.
- Schiff Lai CL, Neuhaus P, Tillman H, et al. Adefovir dipivoxil provides significant clinical benefit, reduces MELD score, and prevents transplantation in chronic hepatitis B patients wait-listed for liver transplantation with lamivudine resistance. J Hepatol 2005;42(suppl 2):5.
- Perrillo R, Hann HW, Mutimer D, et al. Adefovir dipivoxil added to ongoing lamivudine in chronic hepatitis B with YMDD mutant hepatitis B virus. Gastroenterology 2004;126:81–90.
- Dienstag JL,Wei LJ, Cross A, et al Entecavir is superior to lamivudine and adefovir in trials of HBeAg-positive and negative chronic hepatitisBinfection:Across-study analysis with published reports. J Hepatol 2005;42(suppl 2):174.
- 2004 Red book of average wholesale drug prices. Montvale, NJ: Thompson Medical Economics, 2004.
- RxNews newsletter: FDAupdate.Available at: http://www.rxsolutions.com/b/rxnews/rxnews view.asp?Article=571&type=18. (Accessed June, 2005).
- FDA’s approval of Baraclude signals new option for chronic hepatitis B. Available at: http://www.aishealth.com/Bnow/051105c.htm. (Accessed June,2005).
- Kanwal F, Gralnek IM, Martin PM, et al. Treatment alternatives for chronic hepatitis B virus infection: A costeffectiveness analysis. Ann Intern Med 2005;142:821–31.
- Gold MR, Siegel JE, Russell LB, et al eds. Costeffectiveness in health and medicine. New York, NY: Oxford University Press, 1996.
- D’Amico G, Morabito A, Pagliaro L, et al. Survival and prognostic indicators in compensated and decompensated cirrhosis. Dig Dis Sci 1986;31:468–75.
- Di Marco V, Iacono OL, Camma C, et al. The long-term course of chronic hepatitis B. Hepatology 1999;30:257–64.
- Brunetto MR, Oliveri F, Coco B, et al. Outcome of anti-HBe positive chronic hepatitisBin alpha-interferon treated and untreated patients: A long termcohort study. J Hepatol 2002;36:263–70.
- Lo KJ, Tong MJ, Chien MC, et al. The natural course of hepatitisBsurface antigen-positive chronic active hepatitis in Taiwan. J Infect Dis 1982;146:205–10.
- Xu B, Hu DC, Rosenberg DM, et al. Chronic hepatitis B: A long-term retrospective cohort study of disease progression in Shanghai, China. J Gastroenterol Hepatol 2003;18:1345–52.
- Sulaiman HA. The development of hepatocellular carcinoma from liver cirrhosis during a follow-up study. Gastroenterol Jpn 1989;24:567–72.
- de Jongh FE, Janssen HL, de Man RA, et al. Survival and prognostic indicators in hepatitis B surface antigenpositive cirrhosis of the liver. Gastroenterology 1992;103:1630–5.
- Thyagarajan SP, Panchandam M, Subramanian S, et al. Duration of hepatitis B surface antigenaemia and its correlation with the histopathological and clinical outcome in acute and chronic hepatitis. J Med Microbiol 1983;16:227–31.
- Benvegnu L, Gios M, Boccato S, et al. Natural history of compensated viral cirrhosis: A prospective study on the incidence and hierarchy of major complications. Gut 2004;53:744–9.
- Weissberg JI, Andres LJ, Smith CI, et al. Survival in chronic hepatitis B. Ann Int Med 1984;101:613–6.
- Craxi A, Colombo P, D’Amico G, et al. Hepatitis B infection and liver cirrhosis: A reappraisal from the Mediterannean area. Ann Ist Super Sanita 1988;24:257–66.
- Papatheodoridis GV, Manesis E, Hadziyannis SJ. The long-term outcome of interferon-alpha treated and untreated patients with HBeAg negative chronic hepatitis B. J Hepatol 2001;34:306–13.
- Fattovich G, Brollo L, Giustina G, et al. Natural history and prognostic factors for chronic hepatitis type B. Gut 1991;32:294–8.
- LiawYF, Sung JJ, ChowWC,et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease.NEngl J Med 2004;351:1521–31.
- Fattovich G, Giustina G, Schalm S, et al. Occurrence of hepatocellular carcinoma and decompensation in Western Eurpoean patients with cirrhosis type B. Hepatology 1995;21:77–82.
- Viola LA, Coleman JC, Fluker JL, et al. Natural history of liver disease in chronic hepatits B surface antigen carriers. A survey of 100 patients from Great Britain. Lancet 1981;2:1156–9.
- Davis GL, Hoofnagle JH. Spontaneous reactivation of chronic hepatitis B virus infection. Gastroenterology 1984;86:230–5.
- Yao FY, Terrault NH, Freise C, et al. Lamivudine treatment is beneficial in patients with severely decompensated cirrhosis and actively replicating hepatitis B infection awaiting liver transplantation:Acomparative study using a matched, untreated cohort. Hepatology 2001;34:411–6.
- Yao FY, Bass NM. Lamivudine treatment in patients with severely decompensated cirrhosis due to replicating hepatitis B infection. J Hepatol 2000;33:301–7.
- Saeed ZA, Stiegmann GV, Ramirez FC, et al. Endoscopic variceal ligation is superior to combined ligation and sclerotherapy for esophageal varices: A multicenter prospective randomized trial. Hepatology 1997;25:71–4.
- Gournay J, Masliah C, Martin T, et al. Isosorbide mononitrate and propranolol compared with propranolol alone for the prevention of variceal rebleeding. Hepatology 2000;31:1239–45.
- Chan HLY, Hui AY,Wong ML, et al. Genotype C hepatitis B virus infection is associated with an increased risk of hepatocellular carcinoma. Gut 2004;53:1494–8.
- Oka H, Kuioka N, Kim K, et al. Prospective study of early detection of hepatocellular carcinoma in patients with cirrhosis. Hepatology 1990;12:680–7.
- Musca A, Cordova C, Barnaba V, et al. HBeAg/Anti-Hbe system and development of primary hepatocellular carcinoma in patients with HBsAg-positive liver cirrhosis. Hepatogastroenterology 1983;30:3–5.
- Nakaumura S, Takezwa Y, Kera K, et al. Survival of and hepatoma development in patients with liver cirrhosis. Tohoku J Exp Med 1982;136:387–9.
- Solomon JA, Weinstein MC, Hammitt JK, et al. Costeffectiveness of treatment for chronic hepatitis C infection in an evolving patient population. JAMA 2003;290:228–37.
- Llovet JM, Bustamante J, Castells A, et al. Natural history of untreated nonsurgical hepatocellular carcinoma: Rationale for the design and evaluation of therapeutic trials. Hepatology 1999;29:62–7.
- Villa E, Moles A, Ferretti I, et al. Natural history of inoperable hepatocellular carcinoma: Estrogen receptors’ status in the tumor is the strongest prognostic factor for survival. Hepatology 2000;32:233–8.
- United Network For Organ Sharing data. Available at: www.UNOS.org. (Accessed April, 2005).
- Rosenau J, Bahr MJ, Tillmann HL, et al. Lamivudine and low-dose hepatitis B immune globulin for prophylaxis of hepatitis B reinfection after liver transplantation possible role of mutations in the YMDD motif prior to transplantation as a risk factor for reinfection. J Hepatol 2001;34:895–902.
- Han SH, Ofman J, Holt C, et al. An efficacy and costeffectiveness analysis of combination hepatitis B immune globulin and lamivudine to prevent recurrent hepatitis B after orthotopic liver transplantation compared with hepatitis B immune globulin monotherapy. Liver Transpl 2000;6:741–8.
- Anselmo DM, Ghobrial RM, Jung LC, et al. New era of liver transplantation for hepatitis B: A 17-year singlecenter experience. Ann Surg 2002;235:611–9.
- Yao FY, Osorio RW, Roberts JP, et al. Intramuscular hepatitis B immune globulin combined with lamivudine for prophylaxis against hepatitis B recurrence after liver transplantation. Liver Transpl Surg 1999;5:491–6.
- Markowitz JS, Martin P, Conrad AJ, et al. Prophylaxis against hepatitis B recurrence following liver transplantation using combination lamivudine and hepatitisBimmune globulin. Hepatology 1998;28:585–9.
- Angus PW, McCaughan GW, Gane EJ, et al. Combination low-dose hepatitisBimmune globulin and lamivudine therapy provides effective prophylaxis against posttransplantation hepatitis B. Liver Transpl 2000;6:429–33.
- Girlanda R, Mohsen AH, Smith H, et al. Hepatitis B virus genotype A and D and clinical outcomes of liver transplantation for HBV-related disease. Liver Transpl 2004;10:58– 64.
- Machicao VI, Soldevilla-Pico C, Devarbhavi HC, et al. Hepatitis B liver transplant patients on combination of lamivudine and high dose IV immune globulin has less significant histological progression than hepatitis C transplanted patients. Hepatology 2001;34:411A.
- Marzano A, Salizzoni M, Debernardi-Venon W, et al. Prevention of hepatitis B virus recurrence after liver transplantation in cirrhotic patients treated with lamivudine and passive immunoprophylaxis. J Hepatol 2001;34:903–10.
- Yoshida EM, Erb SR, Partovi N, et al. Liver transplantation for chronic hepatitis B infection with the use of combination lamivudine and low-dose hepatitisBimmune globulin. Liver Transpl Surg 1999;5:520–5.
- McCaughan GW, Spencer J, Koorey D, et al. Lamivudine therapy in patients undergoing liver transplantation for hepatitis B virus precore mutant-associated infection: High resistance rates in treatment of recurrence but universal prevention if used as prophylaxis with very low dose hepatitis B immune globulin. Liver Transpl Surg 1999;5:512–9.
- Lee PH, Hu RH, Tsai MK, et al. Liver transplantation for patients with hepatitis B: Prevention of hepatitis B recurrence by intravenous antihepatitis B immunoglobulin and lamivudine. Transplant Proc 2000;32:2245–7.
- Roche B, Samuel D, Roque AM, et al. Intravenous anti HBs Ig combined with oral lamivudine for prophylaxis against HBV recurrence after liver transplantation. J Hepatol 1999;30(suppl 1):80.
- Andreone P, Grazi GL, Gramensi A, et al. Lamivudine plus HBIG combination therapy compared to HBIG or no therapy in preventing hepatitis B recurrence after liver transplantation. J Hepatol 2000;32(suppl 2):51.
- Buti M, Mas A, Prieto M, et al. A randomized study comparing lamivudine monotherapy after a short course of hepatitis B immune globulin (HBIg) and lamivudine with long-term lamivudine plus HBIg in the prevention of hepatitis B virus recurrence after liver transplantation. J Hepatol 2003;38:811–7.
- Perrillo R, Rakela J, Dienstag J, et al. Multicenter study of lamivudine therapy for hepatitis B after liver transplantation. Lamivudine Transplant Group. Hepatology 1999;29:1581–6.
- Mutimer D, DusheikoG, Barrett C, et al. Lamivudine without HBIg for prevention of graft reinfection by hepatitis B: Long-term follow-up. Transplantation 2000;70:809–15.
- Samuel D, Muller R, Alexander G, et al. Liver transplantation in European patients with the hepatitis B surface antigen. N Engl J Med 1993;329:1842–7.
- Terrault NA, Zhou S, Combs C, et al. Prophylaxis in liver transplant recipients using a fixed dosing schedule of hepatitis B immunoglobulin. Hepatology 1996;24:1327– 33.
- Huang EJ, Wright TL, Lake JR, et al. Hepatitis B and C coinfections and persistent hepatitis B infections: Clinical outcome and liver pathology after transplantation. Hepatology 1996;23:396–404.
- Mutimer D, Pillay D, Shields P, et al. Outcome of lamivudine resistant hepatitis B virus infection in the liver transplant recipient. Gut 2000;46:107–13.
- Schiff E, Dienstag JL, Karayalcin S, et al. Lamivudine and 24weeks of lamivudine/interferon combination therapy for hepatitis B e antigen-positive chronic hepatitis B in interferon nonresponders. J Hepatol 2003;38:818–26.
- Lai CL, Dienstag J, Schiff E, et al. Prevalence and clinical correlates of YMDD variants during lamivudine therapy for patients with chronic hepatitis B. Clin Infect Dis 2003;36:687–96.
- Tassopoulos NC, Volpes R, Pastore G, et al. Efficacy of lamivudine in patients with hepatitis B e antigen-negative hepatitis B virus DNA-positive (precore mutant) chronic hepatitis B. Hepatology 1999;29:889–96.
- Lai CL, Chien RN, Leung NW, et al. A one-year trial of lamivudine for chronic hepatitis B. Asia Hepatitis Lamivudine Study Group. N Engl J Med 1998;339:61–8.
- Lee HC, Suh DJ, Ryu SH, et al. Quantitative polymerase chain reaction assay for serum hepatitis B virus DNA as a predictive factor for post-treatment relapse after lamivudine induced hepatitis B e antigen loss or seroconversion. Gut 2003;52:1779–83.
- Chein RN, Yeh CT, Tsa SL, et al. Determinants for sustained HBeAg response to lamivudine therapy. Hepatology 2003;38:1267–73.
- Van Nunen AB, Hansen BE, Suh DJ, et al. Durability of HBeAg seroconversion following antiviral therapy for chronic hepatitis B: Relation to type of therapy and pretreatment serum hepatitis B virus DNA and alanine aminotransferase. Gut 2003;52:420–4.
- Papatheodoridis GV, Dimou E, Laras A, et al. Course of virologic breakthroughs under long term lamivudine in HBeAg-negative precore mutant HBV liver disease. Hepatology 2002;36:219–26.
- Lau DT-Y, Khokhar F, Doo E, et al. Long-term therapy of chronic hepatitis B with lamivudine. Hepatology 2000;32:828–34.
- Buti M, Cotrina R, Jardi R, et al. Two years of lamivudine therapy in anti-HBe-positive patients with chronic hepatitis B. J Viral Hepatitis 2001;8:270–5.
- Di Marco V, Marzano A, Lampertico P, et al. Clinical outcome of HBeAg-negative chronic hepatitis B in relation to virological response to lamivudine. Hepatology 2004;40:883–91.
- Santantonio T, Mazzola M, Iacovazzi T, et al. Long-term follow-up of patients with anti-HBe/HBV DNA-positive chronic hepatitis B treated for 12 months with lamivudine. J Hepatol 2000;32:300–6.
- Santantonio T, Niro GA, Sinisi E, et al. Lamivudine/interferon combination therapy in anti-Hbe positive chronic hepatitis B patients: A controlled pilot study. J Hepatol 2002;36:799–804.
- Fung SK, Wong F, Hussain M, et al. Sustained response after a 2-year course of lamivudine treatment for hepatitis B e antigen-negative chronic hepatitis B. J Viral Hepat 2004;11:432–8.
- Hadziyannis SJ, Paptheodoridis GV, Dimou E, et al. Efficacy of long-termlamivudine monotherapy in patients with hepatitis B e antigen-negative chronic hepatitis B. Hepatology 2002;32:847–51.
- Lampertico P, Vigano M, Iavarone M, et al. The long-term outcome of HBeAg-negative patients with cirrhosis treated with lamivudine monotherapy:A5-year prospective cohort study. Hepatology 2004;40:674A.
- Kapoor D, Guptan RC, Wakil SM, et al. Beneficial effects of lamivudine in hepatitis B virus related decompensated cirrhosis. J Hepatol 2000;33:308–12.
- Marzano A, Lampertico P, Mazzaferro V, et al. Prophylaxis of hepatitis B virus recurrence after liver transplantation in carriers of lamivudine-resistant mutants. Liver Transpl 2005;11:532–8.
- Locarnini S, Qi X, Arterburn S, et al. Incidence and predictors of emergence of adefovir resistant HBV during four years of adefovir dipivoxil therapy for patients with chronic hepatitis B. 40th Annual Meeting of the European Association for the Study of the Liver (EASL);volume pending: Abs# 36.
- Schiff ER, Lai CL, Hadziyannis S, et al. Adefovir dipivoxil therapy for lamivudine-resistant hepatitis B in pre- and post-liver transplantation patients. Hepatology 2003;38:1419–27.
- Schiff ER, Lai CL, Neuhaus P, et al. Long-term safety and efficacy of adefovir dipivoxil in the treatment of chronic hepatitis B in patients with pre- and post-liver transplantation with lamivudine resistant hepatitisBvirus. Hepatology 2004;40:660A.
- Consigny Y, Plessier A, Martinot M, et al. Predictors of a pejorative outcome in patients treated with adefovir dipivoxil for reactivation of chronic hepatitis B due to lamivudine resistant hepatitis B virus mutants. 40th Annual Meeting of the European Association for the Study of the Liver (EASL);volume pending: Abs#:479.
- Lampertico P, Vigano M, Manenti E, et al. Twenty four months combination therapy with adefovir dipivoxil and lamivudine in lamivudine resistant patients with HBeAgnegative chronic hepatitis B. J Hepatol 2005;42(suppl 2):182.
- Chong CA, Gulamhussein A, Heathcote EJ, et al. Healthstate utilities and quality of life in hepatitis C patients. Am J Gastroenterol 2003;98:630–8.
- American Medical Association. AMA CPT code book 2004.
- Bennett WG, Inoue Y, Beck JR, et al. Estimates of the costeffectiveness of a single course of interferon-alpha 2b in patients with histologically mild chronic hepatitis C. Ann Intern Med 1997;127:855–65.
- United States Department of Labor Bureau of Labor Statistics. Consumer price index calculator Available at: www.bls.gov. (Accessed December, 2004).
- Muennig P. Designing and conducting cost-effectiveness analyses in medicine and health care. San Francisco: Jossey-Bass, 2002.
- Briggs AH, O’Brien BJ, Blackhouse G. Thinking outside the box: Recent advances in the analysis and presentation of uncertainty in cost-effectiveness studies. Annu Rev Public Health 2002;23:377–401.
- Baraclude_ [package insert]. Manufacturer location: name, 2005.
- Lieu TA, Gurley RJ, Lundstrom RJ, et al. Projected costeffectiveness of primary angioplasty for acute myocardial infarction. J Am Coll Cardiol 1997;30:1741–50.
- Moore RD, Chiasson RE. Cost-utility analysis of prophylactic treatment with gancyclovir for cytomegalovirus retinitis. J Acquir Immune Defic Syndr Hum Retrovirol 1997;16:15–21.
- Spiegel BMR, Targownik LE, Dulai GS, et al. The cost-effectiveness of cyclooxygenase-2 selective inhibitors in the management of chronic arthritis. Ann Int Med 2003;138:795–806.
- Chapman RH, Stone PW, Sandberg EA, et al. A comprehensive league table of cost-utility ratios and a sub-table of “panel-worthy” studies. Med Decis Making 2000;20:451–67.
- Petitti DB. Meta-analysis, decision analysis, and costeffectiveness analysis: Methods for quantitative synthesis in medicine. New York: Oxford University Press, 2000.
- Marcellin P, Chang TT, Lim SG, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigen-positive chronic hepatitis B. N Engl J Med 2003;348:808–16.
- Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Adefovir dipivoxil for the treatment of hepatitis B e antigennegative chronic hepatitis B. N Engl J Med 2003;348:800–7.
- Buti M, Esteban R, D’Hebron V, et al. Continued efficacy and safety of adefovir dipivoxil in chronic hepatitis B patients with lamivudine resistant HBV: 1-year results.Hepatology 2004;40:671A.
- Colonno RJ, Rose RE, Levine K, et al. Entecavir resistance is not observed in nucleosid-na¨ıve subjects and is observed infrequently by week 48 in lamivudine refractory subjects with chronic HBV infection. J Hepatol 2005;42(suppl 2):173.
- Gish RG, De Amn RA, Pedersen C, et al. Sustained response off-treatment to entecavir and lamivudine after 48 weeks of treatment in nucleoside-na¨ıve, HbeAg positive patients: 24-week follow up results of phase 3 study ETV-022. J Hepatol 2005; 42(suppl 2):177.
- Thomas HC, Manns PM, Gish RG, et al. Decline in serum HBV DNA and ALT normalization is associated with histological response among nucleoside na¨ıve patients in entecavir phase III trials. J Hepatol 2005; 42(suppl 2):192–3.
- Manns MP, Raptopoulou-Gigi M, Sollano J, et al. Entecavir is well tolerated for the treatment of nucleoside na¨ıve and lamivudine refractory chronic hepatitis B: Phase II/III safety results. J Hepatol 2005; 42(suppl 2):185.
- Lai CL, Shouval D, Lok AS, et al. Entecavir versus lamivudine for patients with HBeAg-negative chronic hepatitis B. N Engl J Med 2006;354:1011–20.
- Chang TT, Gish RG, de Man R, et al.Acomparison of entecavir and lamivudine for HBeAg-positive chronic hepatitis B. N Engl J Med 2006;354:1001–10.
- Younossi ZM, Boparai N, McCormick M, et al. Assessment of utilities and health-related quality of life in patients with chronic liver disease. Am J Gastroenterol 2001;96:579– 83.
—— End