")
Source : The Indonesian Journal of Gastroenterology, Hepatology, and Digestive Endoscopy, Vol 12, Number 3, December 2011
Written by : Jeffry Beta Tenggara*, Irsan Hasan**, Andri Sanityoso**, Murdani Abdullah***
* Department of Internal Medicine, Faculty of Medicine, University of Indonesia Dr. Cipto Mangunkusumo General National Hospital, Jakarta, ** Division of Hepatology, Department of Internal Medicine, Faculty of Medicine, University of Indonesia/Dr. Cipto Mangunkusumo General National Hospital, Jakarta, *** Division of Gastroenterology, Department of Internal Medicine, Faculty of Medicine, University of Indonesia/Dr. Cipto Mangunkusumo General National Hospital, Jakarta
ABSTRACT
Background: Indonesia is an endemic country for hepatitis B viral infection. Thus, early diagnosis of cirrhosis is important to be established with regard to prompt treatment and to determine the patients’ prognosis. Liver biopsy which is a gold standard in diagnosing liver cirrhosis has several limitations, such as expensive and invasive. The objective of this study was to identify the accuracy of non-invasive markers: aspartate/alanine transaminase ratio (AAR), age-platelet index (API), aspartate transaminase to platelet ratio index (APRI), spleen to platelet ratio index (SPRI), and age-spleen-platelet ratio index (ASPRI) in predicting cirrhosis in chronic hepatitis B patients.
Method: A diagnostic study was performed in Division of Hepatology and Hepatology Outpatient Clinic, Depatment of Internal Medicine, Cipto Mangunkusumo Hospital between January 2009 and July 2010, with the participation of 71 chronic hepatitis B patients who had undergone liver biopsy consecutively. Stage of fibrosis was determined based on the METAVIR scoring system. Five non-invasive markers: AAR, API, APRI, SPRI, and ASPRI were compared with liver biopsy results. Statistical analysis was performed by using T-test and Spearman correlation test using SPSS version 13.
Results: API, APRI, SPRI, and ASPRI had significant correlation with the incidence of liver cirrhosis in hepatitis B infection (p < 0.05). However, AAR had no correlation with the incidence of cirrhosis. Using the cut-off point of 1.19, APRI was the best marker with area under curve (AUC) 0.91, sensitivity 83.3%, and specificity 89.2%.
Conclusion: Non-invasive markers were suitable in predicting cirrhosis and have the potential to decrease the number of liver biopsy in chronic hepatitis B patients.
Keywords: non-invasive markers, chronic hepatitis B, liver cirrhosis
ABSTRAK
Latar Belakang: Indonesia adalah negara endemis infeksi virus hepatitis B.Oleh sebab itu, diagnosis dini sirosis sangat penting dilakukan dalam hal tatalaksana dan penentuan prognosis dari pasien. Biopsi hati yang merupakan standar baku untuk menegakkan sirosis hati memiliki keterbatasan antara lain mahal dan bersifat invasif. Tujuan dari penelitian ini yaitu untuk mengetahui akurasi petanda non-invasif aspartate/alanine aminotransferase ratio (AAR), age-platelet index (API), aspartate aminotransferase to platelet ratio index (APRI), spleen to platelet ratio index (SPRI) dan age-spleen-platelet ratio index (ASPRI) untuk memprediksi sirosis pada pasien dengan hepatitis B kronik.
Metode: Penelitian ini merupakan penelitian uji diagnostik yang dilakukan di Divisi Hepatologi dan Poliklinik Hepatologi Ilmu Penyakit Dalam Rumah Sakit Cipto Mangunkusumo selama bulan Januari 2009 hingga Juli 2010 dengan melibatkan 71 pasien hepatitis B kronik yang telah melalui biopsi hati secara konsekutif. Stadium fibrosis dinilai berdasarkan sistem skoring METAVIR. Lima petanda non invasif: AAR, API, APRI, SPRI dan ASPRI dibandingkan dengan hasil biopsi hati. Uji T dan uji korelasi Spearman digunakan dengan analisis statistik program SPSS versi 13.
Hasil: API, APRI, SPRI dan ASPRI memiliki korelasi yang signifikan dengan kejadian sirosis pada infeksi hepatitis B (p < 0,05), namun petanda AAR tidak memiliki korelasi dengan kejadian sirosis. Menggunakan nilai batas 1,19, petanda APRI adalah petanda terbaik dengan luas area di bawah kurva 0,91, sensitifitas 83,3% dan spesifisitas 89,2%.
Kesimpulan: Petanda non-invasif dapat digunakan untuk prediksi sirosis dan dapat menurunkan angka biopsi hati pada pasien hepatitis B kronik.
Kata Kunci: petanda non invasif, hepatitis B kronik, sirosis hati
INTRODUCTION
Hepatitis B virus (HBV) infection is the main etiology of acute and chronic liver disease worldwide, which will finally lead to cirrhosis and hepatocelullar carcinoma (hepatoma). Approximately 350 million people experienced chronic infection and between 500,000 and 1.2 million death per year occurred due to hepatitis B associated complications.1 The prevalence of HBV infection in Indonesia and South East Asian countries was 10-20%, mostly acquired perinatally; while the prevalence of HBV infection in Jakarta was reported to be 4.1%.2,3,4 Therefore, liver cirrhosis is important to be detected early to slower the clinical progression of the disease’ and decrease the incidence of complication which may happen with antivirus administration.
Liver biopsy is the gold standard to diagnose liver cirrhosis and plays a part in the management of chronic hepatitis B infection. Consensus on management of hepatitis B in Indonesia 2006 stated that one of the criteria in antivirus administration was the presence of significant degree liver fibrosis.5 Liver biopsy also provides the information on the degree of necroinflammation activity and degree of liver fibrosis, which are required in determining the prognosis and also plays role in identifying other etiologies of liver disease.6,7 However, liver biopsy has some limitations, such as relatively high cost procedure, invasive, high morbidity and mortality risk (3% and 0.03%, respectively), also the bias potency due to sampling error and inter and intraobserver variation which may result in error in determining the degree of fibrosis.8 Liver biopsy facility and histopathologic examination for liver tissue are not available evenly in Indonesia. In regard to the limitations of liver biopsy, a non-invasive method to diagnose liver cirrhosis is required.
Several reported serologic non-invasive markers can be used to predict fibrosis and cirrhosis in hepatitis C, includes aspartate aminotransferase (AST) to alanine aminotransferase (ALT) ratio (AAR), AST-to-platelet ratio index (APRI), and age-platelet count index (API).9 However, the use of non-invasive predictors for hepatitis C cannot be directly implemented in hepatitis B due to the presence of difference in natural progression of the disease, which is associated with different increase of ALT, and histopathological appearance.9,10 Therefore, the objective of this study was to know the accuracy degree of ASPRI, API, SPRI, AAR, and APRI in predicting cirrhosis non-invasively in chronic hepatitis B patients.
METHOD
A diagnostic test study was performed in 71 patients with chronic hepatitis B in Hepatology Outpatient Clinic, Internal Medicine Department, Cipto Mangunkusumo Hospital consecutively between January 2009 and July 2010. Patients with chronic hepatitis B who agreed to participate in this study were included in the study after informed consent has been received. Blood examination, abdomen ultrasonography (USG), and liver biopsy were performed on the same day. Patients with signs of liver decompensation, such as ascites, history of hematemesis, hepatic encephalopathy, Child Pugh class B and C, coagulation disorder, suffered from chronic liver disease due to other etiologies, such as hepatitis C co-infection, under antiviral or hepatoprotector therapy, consuming alcohol, and suffered from other disease causing splenomegaly were not included in this study.
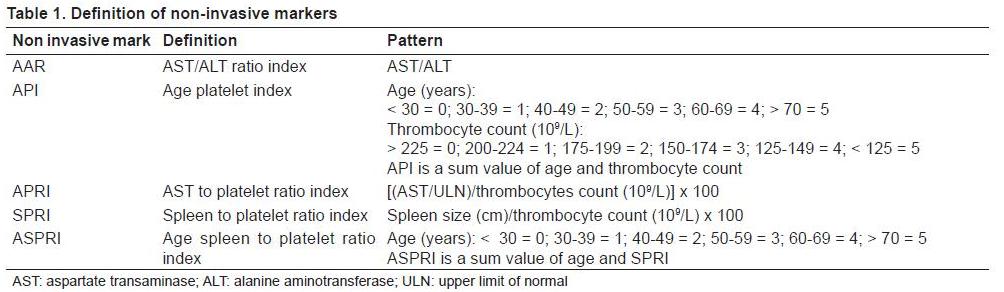
Liver tissue was examined by an anatomy pathologist. Liver fibrosis was determined by using METAVIR criteria, which constitute of no fibrosis found (F0), portal fibrosis without septa (F1), portal fibrosis with septa (F2), many septa without fibrosis (F3), and liver cirrhosis (F4). Meanwhile, blood examination and liver biopsy were performed on the same day. Spleen size was measured by using ultrasonography (USG) by a hepatologist. The longest longitudinal diameter is measured by using electronic measurer in USG monitor. Markers AAR, API, APRI, SPRI, and ASPRI were calculated from the laboratory examination data, age, and spleen USG (Table 1).
SPSS version 13 software was used in statistical analysis of this study. Relationship between these five non-invasive markers: AAR, API, SPRI, APRI, and ASPRI with cirrhosis were analyzed using T-test. P value < 0.05 was assumed as statistically significant. Regression analysis (Spearman correlation test) was conducted to evaluate if those variables were correlated with the presence of cirrhosis. To know the accuracy of variable prediction, receiver operating characteristic (ROC) curve analysis was performed. Difference between areas under ROC curve was used to compare prediction capability of each non-invasive marker. Cut off value was set in the highest point of sum value of sensitivity and specificity.
RESULTS
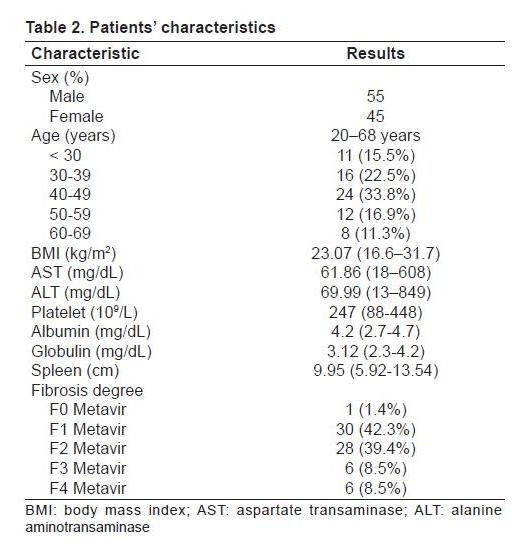
Patients’ clinical and laboratory data were detailed in Table 2. Total analyzed patients were 71 patients, with oldest age group was 40-49 years old. The median value of AST was 61.86 and the median value of ALT was 69.99. Based on degree of fibrosis, most patients were in the F1 group.
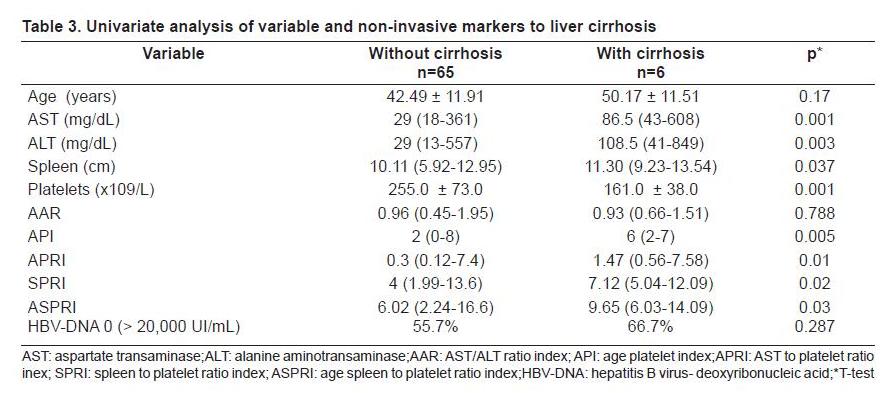
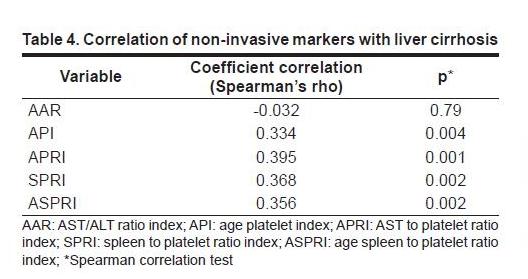
Analysis to variables associated to cirrhosis showed that there was significant difference between cirrhosis and non-cirrhosis group in all analyzed variables (AST, ALT, spleen size, thrombocyte level, API, APRI, SPRI, and ASPRI), except age, AAR, and HBV-DNA (Table 3). In the five non-invasive markers being analyzed, there was significant correlation with the incidence of cirrhosis, except for marker AAR elaborated in Table 4.
ROC curve was prepared to evaluate diagnosis accuracy from those five non-invasive markers in predicting the incidence of liver cirrhosis (Figure 1). Area under the curve (AUC) value to differentiate F4 and F0-F3 from AAR was 0.467 (95% CI = 0.232- 0.702). AUC value from API, APRI, SPRI, and ASPRI were 0.842 (95% CI = 0.658-1.000), 0.910 (95% CI = 0.836-0.985), 0.882 (95% CI = 0.792-0.972), and 0.869 (95% CI = 0.743-0.996), respectively. Based on the area of AUC from the five non-invasive markers being analyzed, AAR has the worst accuracy and APRI has the best accuracy.
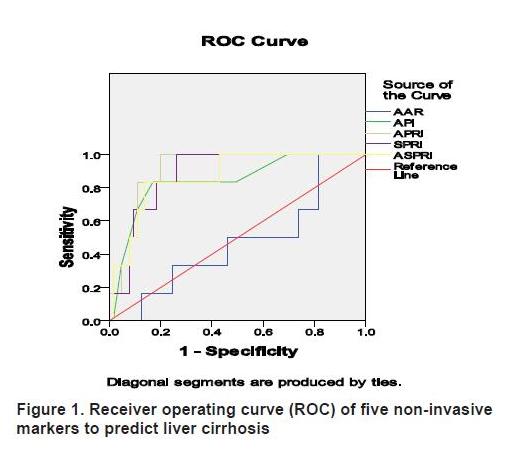
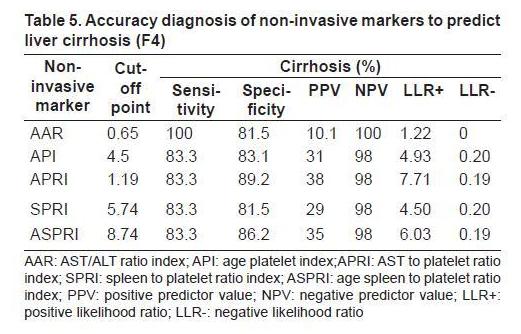
Table 5 revealed the cut off value of those five non-invasive markers, including their sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LLR+), and negative likelihood ratio (LLR-) to predict liver cirrhosis.
DISCUSSION
This study was an initial study with total sample not as big as previous studies and proportion of fibrosis group was less evenly distributed (F4: 8,5%). Correlation analysis between few single variables and non-invasive markers with incidence of cirrhosis showed that AST, ALT, thrombocyte level, spleen size and all non-invasive markers, except AAR had signficant difference statistically between cirrhosis and non-cirrhosis group (p < 0.05). These findings were similar to prospective study results in 125 chronic hepatitis B patients performed by Lee et al, which reported that AST, ALT, platelet, API, and APRI had significant difference between cirrhosis and noncirrhosis group.11
Analysis to association of age variable and AAR marker and HBV-DNA revealed no significant difference between cirrhosis and non-cirrhosis group. Clinical progression of hepatitis B is different from hepatitis C, in which progressive inflammation happens persistently until liver cirrhosis is formed. Differently, the clinical progression of hepatitis B is oftenly accompanied with acute exacerbation, marked by the elevation of AST more to ALT, and followed by inactive period. This explains why age and comparison of AAR were not significantly different between cirrhosis and non-cirrhosis group.10
Thrombocyte level and spleen size are significant predictors to the incidence of cirrhosis. Splenomegaly is a sign occurred due to elevation in portal circulation pressure, causing red pulp spleen congestion. Size of the spleen is the clinical characteristic in chronic liver disease. Study by Aube et al reported that spleen size was associated with portal hypertension due to fibrosis in the liver.12 Thrombocytopenia is one of the liver cirrhosis markers which is caused by thrombopoetin deficiency (TPO). A study showed that there was increase of TPO level and peripheral blood thrombocytes in liver cirrhosis patients after underwent liver transplantation. This proved the role of TPO in the pathophysiology of thrombocytopenia in liver cirrhosis.13 Thrombocyte count is the simplest marker to evaluate liver fibrosis. Decreased thrombocyte count is moderately correlated with the histopathology of fibrosis with correlation coefficient of 0.46-0.5, sensitivity of 77%, and specificity of 88%.14
Analysis between non-invasive markers and incidence of cirrhosis revealed that besides AAR, other markers had significant correlation with cirrhosis. APRI marker had the strongest correlation, followed by marker SPRI, ASPRI, and API (Spearman’s rho 0.395, 0.368, 0.356 and 0.334 with p < 0.05). This result is different from the study conducted by Kim et al, which found out that those five non-invasive markers were correlated with cirrhosis and ASPRI had the strongest correlation.9 However, the result of retrospective study by Yilmaj et al in patients with chronic hepatitis B, chronic hepatitis C, and non-alcoholic fatty liver, exhibited that APRI showed higher accuracy in determining liver fibrosis in chronic hepatitis C patients compared to chronic hepatitis B patients.15
With the cut off value of 0.65, AAR marker showed best results with sensitivity 100%, specificity 18,5%, AUC 0.467, PPV 10.1%, NPV 100%, positive likelihood ratio 1.22 and negative likelihood ratio 0. Based on those values, it could be interpreted that AAR has low AUC and does not provide any additional information in the diagnosis of liver cirrhosis. Elevation of AST in advanced liver fibrosis is caused by decreased AST clearance and mitochondria destruction which leads to relative elevation of AST compared to ALT. However, chronic hepatitis B infection is oftenly accompanied with acute exacerbation, marked by more elevated AST compared to AST. Thus, the AST/ALT ratio could not be used as an accurate marker in predicting liver cirrhosis in chronic hepatitis B infection.
In API marker, using the cut off value of 4.5 best results were obtained, with sensitivity 83.3%, specificity 83.1%, AUC 0.842, PPV 31%, NPV 98%, positive likelihood ratio 4.93, and negative likelihood ratio 0.20. Based on those values, it could be interpreted that API had good AUC, and patient with F4 had 4.93 higher possibility to give value > 4.5 compared to patients with F0-F3. Probability of patients with F4 to get value < 4.5 is 0.2 compared to patients with F0-F3.
In APRI marker, using cut off value of 1.19, best results were obtained with sensitivity 83.3%, specificity 89.2%, AUC 0.91, PPV 38%, NPV 98%, positive LLR 7.71, and negative LLR 0.19. Based on these values, it could be interpreted that APRI had highest and best AUC among other non-invasive markers. Patients with F4 had 7.71 times higher possibility to give value > 1.19 compared to patients with F0-F3. The possibility of patients with F4 to have value < 1.19 is 0.19 times compared to patients with F0-F3.
In SPRI marker, using the cut off value 5.74, best results were obtained with sensitivity 83.3%, specificity 81.5%, AUC 0.882, PPV 29%, NPV 98%, positive LRR 4.5, and negative LRR 0.2. Based on these values, it could be interpreted that SPRI had good AUC, and patients with F4 had 4.5 times higher possibility to give out value of > 5.74 compared to patients with F0-F3. The possibility of patients with F4 to get value < 5.74 was 0.2 times compared to patients with F0-F3. The accuracy of SPRI was the lowest compared to the other four analyzed non-invasive markers.
In ASPRI marker, best results of non-invasive markers predicting F4 was obtained using the cut off value of 8.74, with sensitivity 83.3%, specificity 86.2%, AUC 0.869, PPV 35%, NPV 98%, positive LLR 6.03, and negative LLR 0.19. Based on these values, it could be interpreted that ASPRI had the best AUC, and F4 patients had 6 times higher possibility to give value > 8.74 compared to F0-F3 patients. The possibility of F4 patient to give value < 8.74 was 0.2 times compared to F0-F3 patients.
Study on non-invasive markers to predict cirrhosis in hepatitis B which was conducted by Kim et al in Korea, showed that formula such as ASPRI, API, SPRI could be used to predict or exclude the incidence of cirrhosis with quite high accuracy.9 Kim et al, revealed that from those five non-invasive markers, APRI had the worst accuracy with AUC under 0.8 and ASPRI was the best marker with AUC 0.908. Differently, in this study, APRI was the best non-invasive markers from those five non-invasive markers with AUC 0.91 and AAR was the worst marker with AUC 0.467 and could not be used to evaluate liver cirrhosis.9
PPV values in those further analyzed four invasive markers were low, though it has quite high specificity for each cut off point. This was because PPV was a post-test probability influenced by low prevalence of F4 (pretest probability), specifically 8%.
Result of this study is different with the study conducted by Kim et al and Wai et al, particularly for marker AAR and APRI. This was because of some reasons, such as this study was an introduction study with lesser participants compared to the other two previous studies; other difference could be caused by the previous use of hepatoprotector. Furthermore, studies by Kim et al and Wai et al were performed retroscpectively and thus, the use of hepatoprotector could not be eliminated; while in this study there was wash out period of 2 weeks before the study.9.16 Use of hepatoprotector may alter the transaminase enzyme level which could affect markers AAR and APRI. Other difference which could have influenced the result of the study was the profile age of the subjects, in which the age of the subjects in this study is older compared to the subjects in the study of Kim et al.9 Age affects the clinical progression, in which there was higher incidence of acute exacerbations in younger age.
CONCLUSION
Based on the analysis of this study, it can be concluded that non-invasive markers give out good result to be used as exclusion tests to exclude cirrhosis because of its high sensitivity and NPV value. As a diagnostic tool of cirrhosis, non-invasive markers still has limitations, because of the low PPV value as an effect of low prevalence of cirrhosis among chronic hepatitis B patients.
REFERENCES
- Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment, and current and emerging prevention and control measures. J Viral Hepatol 2004;11:97-107.
- Dienstay JL, Isselbacher KJ. Chronic hepatitis. In: Kasper DL, Fauci AS, Longo DL, Braunwald E, Hauser SL, eds. Harrison’s Principles of Internal Medicine. 16th ed. New York: McGraw-Hill 2003.p.1844-54.
- Soemohardjo S, Gunawan S. Hepatitis B kronik. In: Sudoyo AW, Setiyohadi B, Alwi I, Setiati S, eds. Buku Ajar Ilmu Penyakit Dalam. 4th ed. Jakarta: Pusat Penerbitan Ilmu Penyakit Dalam FKUI 2006.p.435-40.
- Akbar N, Basuki B, Noer HM. Ethnicity, socio-economic status, transfusions and risk of hepatitis B and hepatitis C infection. J Gastroenterol Hepatol 1997;12:752-7.
- Perhimpunan Peneliti Hati Indonesia (PPHI). Panduan tatalaksana infeksi hepatitis B kronik. Konsensus Penatalaksanaan Hepatitis B Indonesia. Jakarta: PPHI 2006.p.6-39.
- Lok AS, McMahon B. AASLD practice guidelines: chronic hepatitis B. Hepatology 2007;45:507-39.
- Bravo AA, Sheth SG, Chopra S. Liver biopsy. N Engl J Med 2001;344:495-500.
- Piccinino F, Sagnelli E, Pasquale G, Giusti G. Complications following percutaneous liver biopsy: a multicentre retrospective study on 68,276 biopsies. J Hepatol 1986;2:165-73.
- Kim BK, Kim SA, Park YN, Cheong JY, Kim HS, Park JY, et al. Non-invasive models to predict liver cirrhosis in patients with chronic hepatitis B. Liver Int 2007;27:969-76.
- Liu CJ, Kao JH, Chen DS. Therapeutic implications of hepatitis B virus genotypes. Liver Int 2005;25:1097–107.
- Lee KG, Seo YS, An H, Um SH, Jung ES, Keum B, et al. Usefulness of non-invasive markers for predicting liver cirrhosis in patients with chronic hepatitis B. J Gastroenterol Hepatol 2010;25:94-100.
- Aube C, Oberti F, Korali N. Ultrasonographic diagnosis of hepatic fibrosis or cirrhosis. J Hepatol 1999:30;472–8.
- Radosavljevic MP, Wichlas M, Zacherl J, Stiegler G, Stohlawetz P, Fuchsjager M, et al. Thrombopoietin induces rapid resolution of thrombocytopenia after orthotopic liver transplantation through increased platelet production. Blood 2000;95:795-801.
- Lackner C, Struber G, Liegl B. Comparison and validation of simple non-invasive tests for prediction of fibrosis in chronic hepatitis C. Hepatology 2005;41:1376-82.
- Yilmaj Y, Yonal O, Kurt R, Bayrak M, Aktas B, Ozdogan O. Non-invasive assessment of liver fibrosis with the aspartate transaminase to platelet ratio index (APRI): usefulness in patients with chronic liver disease-APRI in chronic liver disease. Hepat Mon 2011;11:103-6.
- Wai CT, Cheng CL, Wee A, Dan YY, Chan E, Chua W, et al. Non-invasive models for predicting histology in patients with chronic hepatitis B. Liver Int 2006;26:666-72
Correspondence:
Jeffry Beta Tenggara
Department of Internal Medicine
Dr. Cipto Mangunkusumo General National Hospital
Jl. Diponegoro No. 71 Jakarta 10430 Indonesia
Phone: +62-21-31930956 Facsimile: +62-21-3914830
E-mail: jefrry.tenggara@yahoo.com
———- End