")
Written by: dr. Irsan Hasan Sp.Pd, KGEH ( Division of Hepatology, Department of Internal Medicine, Faculty of Medicine, University of Indonesia-Dr. Cipto Mangunkusumo Hospital, Jakarta )
Source : Acta Med Indonesia – Indonesia Journal International Medicine , Vol 37 – Number 4 – October – December 2005
INTRODUCTION
Hepatitis B virus (HBV) is a serious public health problem and a cause of infectious disease mortality worldwide. Each year over 1 million people die from HBV related chronic liver disease, including cirrhosis and hepatocellular carcinoma (HCC). Hepatocellular carcinoma is one of the most common cancers worldwide, and HBV is responsible for at least 75% of these cancers.1,2 The relative ease with which HBV antigens and antibodies can be assayed has greatly expedited study of the transmission and epidemiology of this disease. In developing countries, acute hepatitis B is a frequent cause of jaundice in adults and accounts for about 50 percent of cases of acute viral hepatitis. In contrast, in undeveloping contries, HBV infection is an almost universal infection of childhood and the HBsAg carrier state affects 5 to 15 percent of adults.3 Because of the high HBV related morbidity and mortality, the global disease burden of hepatitis B is substansial.
EPIDEMIOLOGY
It is estimated that approximately 2 billion people–one third of the world’s population have serological evidence of past or present HBV infection, and more than 350 million people are chronically infected.4 Approximately 75% of chronic carriers live in Asia and the Western Pacific. It was reported that 15-40% of HBV infected patients would develop cirrhosis, liver failure, or HCC, and 500,000 to 1.2 million people die of HBV infection annually.5 The prevalence of chronic HBV infection varies greatly in different parts of the world. The prevalence of chronic HBV infection worldwide could be categorized as high, intermediate and low endemicity. The age at the time of infection is associated with the endemicity of HBV infection5 (Table 1).
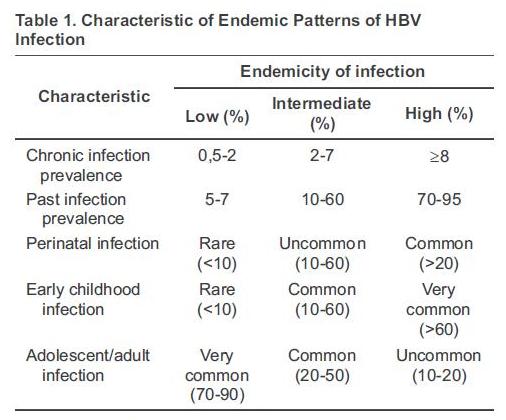
Hepatitis B is highly endemic in developing regions with large population such as South East Asia, China, sub-Saharan Africa and the Amazon Basin, where at least 8% of the population are HBV chronic carriers. In these areas, 70-95% of the population show past or present serological evidence of HBV infection. Most infections occur during infancy or childhood. Since most infections in children are asymptomatic, there is little evidence of acute disease related to HBV, but the rates of chronic liver disease and liver cancer in adults are high.5,6
In part of Eastern and Southern Europe, the Middle East and Japan hepatitis B is moderately endemic. Between 10-60% of the population have evidence of infection, and 2-7% are chronic carriers. Acute disease related to HBV is common in these areas because many infections occur in adolescents and adults; however, the high rates of chronic infection are maintained mostly by infections occurring in infants and children. In these areas, mixed patterns of transmission exist, including infant, early childhood and adult transmission.5
The endemicity of HBV is low in most developed areas, such as North America, Northern and Western Europe and Australia. In these regions, HBV infects 5-7% of the population, and only 0.5-2% of the population are chronic carriers. In these areas, most HBV infections occur in adolescents and young adults in relatively well-defined high-risk groups, including injection drug user, homosexual males, health care workers, patients who require regular blood transfusion or hemodialysis.5,7
In Indonesia which has very large areas and consists of thousand of islands with many races and cultures, the endemicity varies greatly. Approximately 3.5% to 9.1% HBsAg prevalence was found in general population in Indonesia, with mean 5.1% (Tables 2 and 3). According to those data, epidemiologically Indonesia could be categorized as an intermediate to highly endemic country.8

TRANSMISSION AND THE CARRIER STATE
Transmission of HBV is largely from the parenteral or inapparent parenteral route. Blood is the most important vehicle for transmission, but other body fluids have also been implicated. Currently, three modes of HBV transmission have been recognized: perinatal, sexual and parenteral/percutaneous transmission.5 The risk of perinatal HBV transmission has been well described. This is greatest for infants born to women who are HBeAg positive and ranges from 70-90% at 6 months of age; about 90% of these children remain chronically infected.
The risk of perinatal infection among infants born to HBeAg negative mothers ranges from 10-40%, with 40-70% of these infected infants remaining chronically infected. Children born to HBsAg positive mothers who do not become infected during the perinatal period remain at high risk of infection during early childhood. In one study, 40% of infants born to HBeAg negative mothers became infected by 5 years of age.1 Another study that was conducted in Jakarta conclude that HBV infection among children is at least 2.5 times more likely due to a transmission in childhood rather than a perinatal transmission.9
Sexual transmission of hepatitis B is a major source of infection in all areas of the world, especially in the low endemic areas. Hepatitis B is considered to be a sexually transmitted disease. For a long time, homosexual men have been considered to be at the highest risk of infection due to sexual contact (70% of homosexual men were infected after 5 years of sexual activity). However, heterosexual transmission accounts for an increasing proportion of HBV infections.1,5
Transmission of HBV via transfusion of blood and plasma derived products has been eliminated in most countries through donor screening for HBsAg and viral inactivation procedures. However, transmission also occurs with inadequately sterilized needles and medical instruments. In the United States and Western Europe, injection drug use remains a very important mode of HBV transmission. Risk of acquiring infection increases with duration of injection drug use.5 In our study HBsAg positive prevalence among drug users was 9.9%, which is 2.5 times greater than in general population.10
Hepatitis B is also spread by intimate contact that is not apparently sexual or parenteral. Thus non sexual intrafamilial spread does occur. Non sexual intrafamilial spread is best described as inapparent parenteral spread, the vehicle perhaps being saliva, blood-tinged fluid, and fluid from open sores, skin lesions, or scratches. Thus the nonsexual spread of hepatitis B in families as appears to occur in underdeveloped areas of the world, is partially unexplained.11 An epidemiological study on HBV in Jakarta found among 21 households with HBsAg positive, 15 had only 1 case and the other 6 (28%) with 2 or more cases for each household. The positive HBsAg was more prevalent among households with 5 persons or more.12
Most persons with chronic HBV infection are not aware that they are infected. These silent carriers are the most likely source of infection to their families and partners. The carrier state is defined on the basis of longitudinal studies as persistence of HBsAg in the circulation for more than 6 months. The carrier state may be lifelong and associated with liver damage varying from minor changes in the nuclei of hepatocytes to persistent hepatitis, chronic hepatitis, cirrhosis, and HCC.11
Several risk factors have been identified in relation to the development of the carrier state. It is more common in men, more likely to follow infections acquired in childhood than those acquired in adult life, and more likely to occur in patients with natural or acquired immune deficiencies. A carrier state becomes established in approximately 5% to 10% of infected adults.11
HBV Genotype
Hepatitis B virus has been classified into 8 genotypes (A-H) based on intergroup divergence of 8% or more in the complete nucleotide sequence. Most HBV genotypes have distinct geographic distributions (Table 4). In brief, genotypes B and C are prevalent in Asia, whereas genotypes A and D prevail in Western countries and India. Genotype E is restricted to Africa, genotype F and H is found in Central and South America. Genotype G has been identified in France and North America.5,13,14
It is noted that genotypes B and C are prevalent in highly endemic areas, such as Asian countries, where vertical or perinatal transmission plays an important role in spreading the virus, whereas genotypes A, D, E, F, G and H are frequently found in areas where horizontal transmission is the main route of infection. Whether the modes of transmission correlate with HBV genotypes awaits further studies.14,15
Although the serological and genotypic classifications of HBV have been documented for a while, the effect of genotypes on the clinical outcome of chronic HBV infection remained unclear. Several studies reported a correlation of HBV genotypes with HBeAg clearance, liver damage, and the response to treatment. It was reported that HBeAg carrier status tends to be longer and the prevalence of HbeAg appears higher in genotype C than with genotype B. HBV carriers with genotype B have lower histologic activity scores, and genotype C is more prevalence in patients with cirrhosis. Recently, we found that genotype C in HCC were higher than in chronic hepatitis B came to our hospital, lead to conclusion that natural history of HBV infection with genotype C may be more worse compare to genotype B.5,15,16
OCCULT HEPATITIS B
Occult hepatitis B is defined by the presence of HBV DNA in serum or liver in the absence of HBsAg. Occult HBV infection has been found in patients with HCC, past HBV infection, chronic hepatitis C, and individuals without HBV serological markers. The frequency of the diagnosis depends on the relative sensitivity of HBV DNA assays and the prevalence of HBV infection in the population. Collectively, around 30% to 35% of HBsAg negative subjects with chronic hepatitis with or without HCC have positive serum HBV DNA. A study in Jakarta reported that occult HBV infection is detectable in 25% and 11% among NBNC and anti HCV positive group respectively.5,17,18
The clinical significance of occult HBV infection remains unclear. Occult HBV infection represents a potential transmission source of HBV via blood transfusion or organ transplantation. In addition, occult HBV infection has been associated with cryptogenic chronic hepatitis and hepatocellular carcinoma. Furthermore, some studies suggested that occult hepatitis B might affect responsiveness of chronic hepatitis C to interferon therapy and disease progression.
REFERENCES
- Alter MJ. Epidemiology and prevention of hepatitis B. Semin Liver Dis. 2003;23:39-46.
- Beasley RP. Hepatitis B virus. The major etiology of hepatocellular carcinoma. Cancer. 1988; 61:1942-56.
- Dusheiko G. Hepatitis B. In: Bircher J, Benhamou JP, Mc Intyre N, Rizetto M, Rodes J, eds. Oxford textbook of clinical hepatology. Oxford: Oxford University Pers; 1999. p. 876-95.
- World Health Organization. Hepatitis B. WHO fact sheet 204.2000. http://www.who.int/mediacentre/factsheets/fs204/en/
- Hou J, Lin Z, Gu F. Epidemiology and prevention of hepatitis B virus infection. Int J Med Sci. 2005;2:50-7.
- Alter M. Epidemiology of hepatitis B in Europe and worldwide. J Hepatol. 2003;39:S64-S9.
- McQuillan GM, Townsend TR, Fields HA, Carroll M, Leahy M, Polk BF. Seroepidemiology of hepatitis B virus infection in the United States. Am J Med 1989;87 (suppl 3A):S5-S10.
- Sulaiman HA, Kandun IN, Iswari R, Budihusodo U. Hepatitis B. Jakarta: Yayasan Penerbit IDI; 1995. p. 2-7.
- Widjaja S, Simon S, Ali S, Listiawan I, Widyastuti A, Kurniawati S, Yap SH. Prevalence of hepatitis B and hepatitis C in women of child-bearing age, in neonates and in children below 5 years of age in an urban area in Jakarta, Indonesia. Acta Medica Indonesiana. 1998;30:33-46.
- Gani RA, Budihusodo U, Waspodo A, Lesmana LA, Hasan I, Akbar N, Noer HMS. Seroepidemiology and risk factors of hepatitis B and C virus infections among drug users in Jakarta, Indonesia. Med J Indones. 2002;11:48-55.
- Zuckerman JN, Zuckerman AJ. The epidemiology of hepatitis B. Clinics in Liver Dis. 1999;3:179-88.
- Akbar N, Basuki B, Mulyanto, Garabrant DH, Sulaiman A, Noer HMS. Ethnicity, socioeconomic status, transfusions andrisk of hepatitis B and hepatitis C infection. J Gastroenterol Hepatol.1997;12:752-57.
- Kao JH. Hepatitis B viral genotypes: Clinical relevance and molecular characteristics. J Gastroenterol Hepatol. 2002;17:643-50.
- Kao JH, Chen DS. Global control of hepatitis B virus infection. Lancet Infect Dis. 2002;2:395-403.
- Fung SK, Lok ASF. Hepatitis B virus genotypes: do they play a role in the outcome of HBV infection ? Hepatology. 2004; 40:790-2.
- Hasan I, Gani RA, Sulaiman AS, Lesmana LA, Sulaiman A, Akbar N. Genotype of hepatitis B virus in patients with chronic hepatitis B and hepatocellular carcinoma in Ciptomangunkusumo Hospital, Jakarta (abstract). Presented in15th Asian Pacific Association for the Study of the Liver, Indonesia 2005.
- Lok ASF. Occult hepatitis B virus infection: diagnosis, implications and management ? J Gastroenterol Hepatol. 2004;19: S114-S7.
- Sanityoso A, Gani RA, Hasan I, Budihusodo U, Akbar N, Lesmana LA, Sulaiman A. Occult hepatitis B virus infection in non-B non-C and in anti-HCV positive hepatocellular carcinoma patients. J Gastroenterol Hepatol. 2004;19:A698.
—– End