")
Source : DOI: 10.3857/jkstro.2010.28.2.106
Written by : Bo Kyong Kim M.D (Department of Radiation Oncology, Dankook University College of Medicine, Cheonan, Korea)
ABSTRACT
Reactivation of the hepatitis B virus (HBV) is a well-recognized complication in patients with chronic HBV infection who receive cytotoxic or other immunosuppressive therapy. In cases of patients treated by radiotherapy however, only a few of such reports exist and most of these include the patients previously treated by chemotherapy or transarterial chemoembolization. The results of this study point to a case of a patient with reactivation of HBV after radiotherapy alone. This study shows the possibility of HBV reactivation by partial hepatic irradiation alone hence, special attention should be paid to patients with HBV disease.
Key Words: Liver, Radiotherapy, Hepatitis B virus, Reactivation
|
Submitted April 7, 2010, accepted April 29, 2010,Reprint requests to BoKyong Kim, M.D., Department of Radiation Oncology, Dankook University College of Medicine, San 16-5 Anseo-dong, Cheonan 330-180, Korea Tel: 041)550-6930, Fax: 041)550-2619 E-mail: merdeglas@dankook.ac.kr This work was supported by the 2008 Grant of Dankook University |
In the cases of hepatic irradiation, there are only several reports about HBV reactivation. Moreover, most of those studies include the patients who were previously treated with chemotherapy and/or transarterial chemoembolization (TACE) of the liver tumor.5,6) So, there are little clinical clues for the definite impact of hepatic irradiation on HBV reactivation in spite of some positive experimental results. Radiotherapy is more increasingly used for the liver and peri-hepatic tumors and the evaluation of the relationship between hepatic irradiation and HBV reactivation is strongly needed to decide the prophylactic use of antiviral agents. Therefore, I would report a case of a patient with reactivation of HBV after partial hepatic irradiation alone and show the possibility of HBV reactivation by hepatic irradiation alone.
CASE REPORT
A 79 year-old man, who had diagnosed as chronic HBV liver disease (HBs-Ag (+), HBs-Ab (−)) 40 years ago, was received hepatic wedge resection and cholecystectomy on May, 2006 due to an incidentally detected liver mass on abdominal CT scan. Several lymph nodes enlargement were also detected, but only two enlarged nodes in common hepatic area were excised. Systematic lymph node dissection was not done because of the poor general status and high operative risk of the patient. Histopathological examination revealed lymphoepithelioma- like cholangiocarcinoma on the hepatic mass and one lymph node.
At 1 month after operation, the size of a retropancreatic node was increased and 18F-fluorodeoxyglucose (FDG) uptake was increased on PET-CT scan (Fig. 1). Therefore, radiotherapy was given to the draining abdominal lymph nodes and the metastatic node using 3D-CRT. Radiotherapy was given by three ports (anterior, posterior, and left) upto 45 Gy in 25 fractions from June to July 2006. On the dose-volume analysis, V30 of liver was less than 20% and V20 was 25%. Prior to irradiation, all the liver enzyme levels were within normal range (Child A) and chemotherapy was not added. During radiotherapy, CBC and liver function test were checked every week.
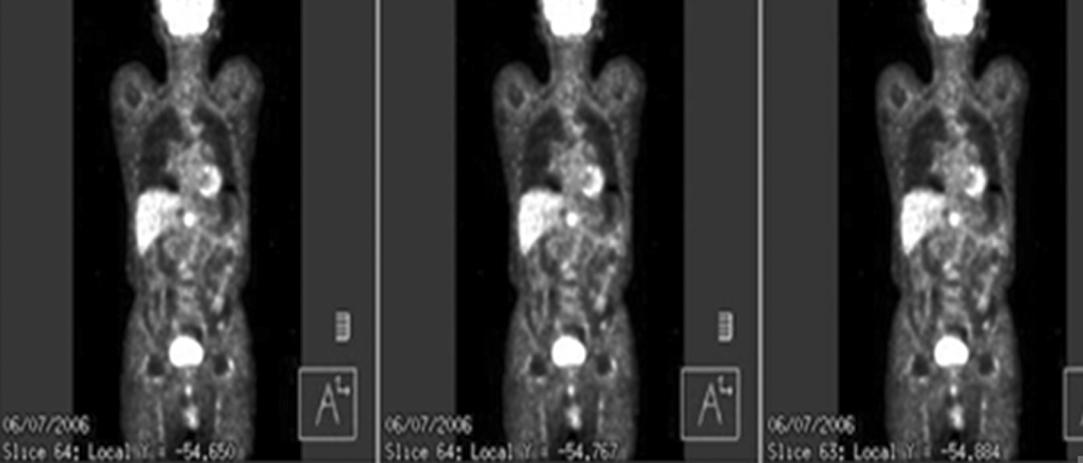
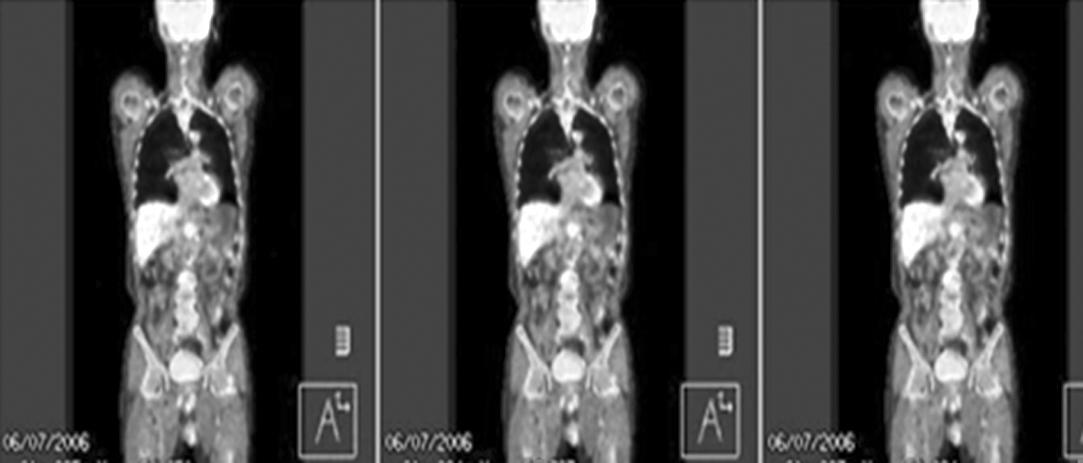


Fig. 1. 18F-fluorodeoxyglucose (FDG) PET/CT scan before abdominal irradiation. At 1 month after surgery, the size of the previously detected retropancreatic node was increased. The node also showed increased 18F-FDG uptake on 18F-FDG PET/CT scan (SUVmax=4.2). The arrows indicate the enlarged lymph node.
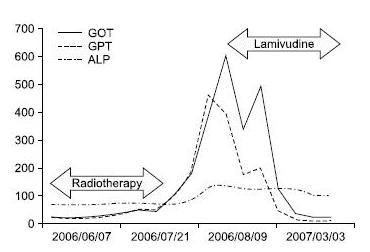
Fig. 2. Sequential changes of the liver enzyme levels. Aspartate aminotransferase (GOT) and alanine minotransferase (GPT) values were slowly increased during radiotherapy and then rapidly increased after radiotherapy. After diagnosis of hepatitis B virus reactivation, antiviral agent (lamivudine) was started and the levels were slowly normalized. ALP: alkaline phosphatase.
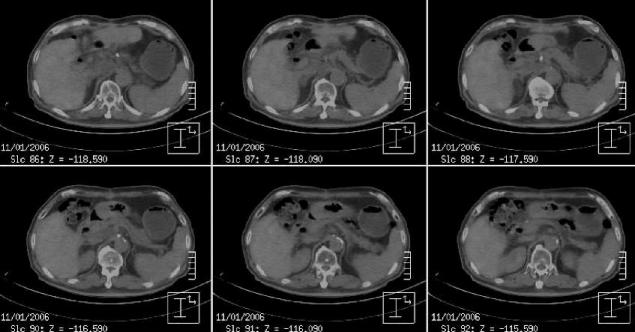
Fig. 3. 18F-fluorodeoxyglucose (FDG) PET/CT scan at 3.5 months after radiotherapy. The increased 18F-FDG uptake on the enlarged node was near completely disappeared.
The response of radiotherapy was remarkable and on 18F-FDG PET/CT scan, there was no increased FDG uptake on the metastatic node at 3.5 month from the end of radiotherapy (Fig. 3) and on abdomen CT scan, it was completely disappeared at 12 months from radiotherapy. There was no evidence of recurrence until 3.5 years follow-up (Fig. 4).
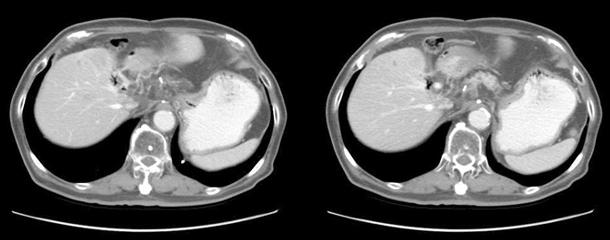
Fig. 4. Abdominal CT scan at 36 months after radiotherapy. At last follow-up, there was no evidence of loco-regional recurrence or distant metastasis.
DISCUSSION
HBV infection and its sequalae are major health problems in the world7) and it is estimated that 400 million people worldwide are HBV carriers.8) HBV infection is endemic in Southeast and East Asia including Korea and there are about 3.5 million HBV carriers in Korea. The natural history of hepatits B is complex and is influenced by many factors, including age at infection, viral factors (HBV genotype, viral mutations, level of HBV replication), host factors (gender, age, immune status) and exogenous factors such as concurrent infection with other hepatotropic viruses or alcohol.4)
HBV reactivation is the well-known complication in the cases of chemotherapy, immunosuppressive therapy after organ transplantation or other benign disease such as Chron’s disease, antituberculosis medications and TACE of liver. In such cases, prophylactic use of antiviral agents is usually recommended. For radiotherapy, however, there are only several reports about HBV reactivation and mostly combined with chemotherapy and/or TACE of the liver tumor.5,6,9) So, there is no recommendation or guidelines of the prophylactic use of antiviral agents in cases of hepatic irradiation for hepatic or peri-hepatic tumors.
Unlikely to HBV reactivation, radiation-induced liver disease (RILD) is well-known complications after radiotherapy of the large volumes of liver. The underlying condition is venoocclusive disease of the small hepatic veins and characterized as anicteric elevation of ALP levels.10) Radiologically, an area of low attenuation is described, which was limited to the radiation portals for conventional doses more than 45 Gy.11) Focal radiation reaction is also observed without any clinical signs of RILD after conventional radiotherapy.12) Herfarth et al.13) reported radiological findings after stereotactic single dose radiotherapy of liver. Three reaction types were found on enhanced CT scans: type 1, hypodense portal-venous phase and isodense late phase, type 2, hypodense portal venous phase and hyperdense late phase, type 3, iso- or hyperdense portal-venous phase and hyperdense late phase. Type 1 and 2 reactions were observed significantly earlier than type 3 and reaction types shifted from type 1 to type 3 during follow-ups. The volume of the reaction also decreases during follow-up. Abnormal liver function test are usually considered as RILD in many cases of radiotherapy. In the HBV endemic areas, however, there are some possibilities of HBV reactivation after hepatic irradiation and some cases of previously considered fatal RILD might be caused by HBV reactivation or RILD combined with HBV reactivation.
In the in vitro experimental model, hepatic irradiation was combined with the increase in both HBV DNA and interleukin-6 (IL-6). IL-6 was produced mainly by irradiated endothelial cells and, in some part, by irradiated normal hepatocytes. Hepatocellular carcinoma cells did not produce IL-6. Such bystander effect might explain the mechanism of HBV reactivation in the cases of hepatic irradiation.14) More recently, animal study also showed that hepatic irradiation combined with IL-6 caused HBV reactivation.15) Such mechanism could also explain the HBV reactivation of the patients who were irradiated liver for the tumors other than hepatocellular carcinoma or other liver tumors. Moreover, such factors associated with HBV reactivation might be used as diagnostic tools or preventive medications in the patients receiving hepatic irradiation.
In this patient, hepatic irradiation alone reactivated HBV and caused severe hepatitis. Therefore, some cares should be given to the patients who had HBV viral disease, when irradiated to the liver not only for hepatic tumors but also for peri-hepatic tumors. Early detection of the HBV reactivation should be made to start the adequate antiviral treatment. Future studies should clarify the patient population according to the previous treatment such as chemotherapy or TACE to evaluate the exact role of hepatic irradiation on HBV reactivation. With such efforts, the relationship between HBV reactivation and hepatic irradiation itself might be clarified and the need for prophylactic antiviral agents might be determined by the actual risk of HBV reactivation by hepatic irradiation alone.
REFERENCES
- Lok AS, Liang RH, Chiu EK, Wong KL, Chan TK, Todd D. Reactivation of hepatitis B virus replication in patients receiving cytotoxic therapy: report of a prospective study. Gastroenterology 1991;100:182-188
- Yeo W, Chan PK, Zhong S, et al. Frequency of hepatitis B virus reactivation in cancer patients undergoing cytotoxic chemotherapy: a prospective study of 626 patients with identification of risk factors. J Med Virol 2000;62:299-307
- Liao CA, Lee CM, Wu HC, Wang MC, Lu SN, Eng HL. Lamivudine for the treatment of hepatitis B virus reactivation following chemotherapy for non-Hodgkin’s lymphoma. Br J Haematol 2002;116:166-169
- Sharma SK, Saini N, Chwla Y. Hepatitis B virus: inactive carriers. Virol J 2005;2:82
- Kim JH, Park JW, Kim TH, Koh DW, Lee WJ, Kim CM. Hepatitis B virus reactivation after three-dimensional conformal radiotherapy in patients with hepatitis B virus-related hepatocellular carcinoma. Int J Radiat Oncol Biol Phys 2007;69: 813-819
- Cheng JC, Wu JK, Lee PC, et al. Biologic susceptibility of hepatocellular carcinoma patients treated with radiotherapy to radiation-induced liver disease. Int J Radiat Oncol Biol Phys 2004;60:1502-1509
- Maddrey WC. Hepatitis B: an important public health issue. J Med Virol 2000;61:362-366
- Lee WM. Hepatitis B virus infection. N Engl J Med 1997;337:1733-1745
- Cheng JC, Liu MC, Tsai SY, Fang WT, Jer-Min Jian J, Sung JL. Unexpectedly frequent hepatitis B reactivation by chemoradiation in postgastrectomy patients. Cancer 2004;101: 2126-2133
- Reed GB Jr, Cox AJ Jr. The human liver after radiation injury: a form of veno-occlusive disease. Am J Pathol 1966; 48:597-611
- Lawrence TS, Robertson JM, Anscher MS, Jirtle RL, Ensminger WD, Fajardo LF. Hepatic toxicity resulting from cancer treatment. Int J Radiat Oncol Biol Phys 1995;31: 1237-1248
- Yamasaki SA, Marn CS, Francis IR, Robertson JM, Lawrence TS. High-dose localized radiation therapy for treatment of hepatic malignant tumors: CT findings and their relation to radiation hepatitis. AJR Am J Roentgenol 1995;165: 79-84
- Herfarth KK, Hof H, Bahner mL, et al. Assessment of focal liver reaction by multiphasic CT after stereotactic singledose radiotherapy of liver tumors. Int J Radiat Oncol Biol Phys 2003;57:444-451
- Chou CH, Chen PJ, Lee PH, Cheng AL, Hsu HC, Cheng JC. Radiation-induced hepatitis B virus reactivation in liver mediated by the bystander effect from irradiated endothelial cells. Clin Cancer Res 2007;13:851-857
- Chou CH, Chen PJ, Jeng YM, Cheng AL, Huang LR, Cheng JC. Synergistic effect of radiation and interleukin-6 on hepatitis B virus reactivation in liver through STAT3 signaling pathway. Int J Radiat Oncol Biol Phys 2009;75:1545-1552.
—– End