")
Source : The Indonesian Journal of Gastroenterology, Hepatology, and Digestive Endoscopy, Vol 11, Number 3, December 2010
Written by : Juwita Sembiring
Department of Internal Medicine, Faculty of Medicine University of North Sumatera/Adam Malik Hospital, Medan
ABSTRACT
Background: Thrombopoetin (TPO) is a cytokine mainly produced in the liver and is the principal regulator in the humoral control mechanism of thrombopoesis. Presumably TPO production is not adequate in patients suffering from severe necroinflammation and advanced liver fibrosis in chronic hepatitis. The aim of this study was to identify the correlation between serum TPO levels and the degree of liver fibrosis.
Method: With analytical cross-sectional design, this sudy analyzed the relationship between the serum TPO level and the degree of liver fibrosis in 62 chronic hepatitis patients from June 2006 to March 2008. The serum level of TPO was examined using the Quantikine human TPO immunoassay, and liver biopsy was performed in accordance to the Metavir scoring system.
Results: There were 22 female and 33 male, with age range from 18 to 70 years old. We found that serum TPO levels were negatively correlated with the degree of liver fibrosis in a very significant fashion (r = -0.284, p < 0.05). At serum TPO level 16.01 pg/mL or lower, the sensitivity and specificity of serum TPO for diagnosing the severity of the fibrosis were the 64.1% and 70.3% respectively, when the disease process was at F3 or greater level (p = 0.003). There was a significant difference between the degree of liver fibrosis and platelet count (p < 0.0001), and significant negative correlation between the degrees of fibrosis with platelet level (r = – 0.783; p = 0.001).
Conclusion: There was a significant negative correlation between serum TPO levels and the degree of liver fibrosis in chronic hepatitis patients and significant negative correlation between the degree of liver fibrosis and platelet count.
Keywords: chronic hepatitis, liver fibrosis, thrombopoietin
INTRODUCTION
Chronic hepatitis is a global problem at present because it frequently progresses to liver cirrhosis and hepatocellular carcinoma that commence with the process of fibrosis in the liver. Liver fibrosis results from chronic damage to the liver associated with excessive accumulation of extracellular matrix proteins. This accumulation will damage the architecture of the liver with fibrous connective tissue formation, which leads to the development of nodules. When the nodules are formed, the condition is called cirrhosis. The main causes of liver fibrosis is a chronic infection from B and C viruses, alcohol drinking, and non-alcoholic steatohepatitis (NASH).1,2,3,4,5
Since fibrosis is known as the major problem causing morbidity and mortality in chronic liver disease, determining the degree of fibrosis is needed to provide early and correct treatment. Liver biopsy as an invasive method is still used as the gold standard in diagnosing the degree of fibrosis. Because many obstacles were experienced with this invasive method, many studies tried to diagnose the degree of fibrosis with noninvasive method.6,7,8,9,10
The difficulties faced are that the clinical picture is not always consistent with the degree of fibrosis and not all patients are willing to undergo a liver biopsy. Since there are many constraints in doing liver biopsy, especially not all places have adequate facilities, so we tried to find whether the determination of trombopoietin (TPO) could be used to predict the severity degree ofliver disease. TPO is a cytokine and also a hormone produced primarily by hepatocyte cells and a little in the kidney, spleen, lung, bone marrow, and brain. TPO strongly induces the proliferation of megakaryocyte (MK). It has been identified as a hormone that controls trombopoiesis.11 TPO is still a relatively new discovery that its utilization must be developed.
This study aimed to obtain data on the correlation of serum TPO levels with the degrees of liver fibrosis and to ascertain whether serum levels of TPO can be used as an alternative to determine the degree of liver fibrosis in patients with chronic hepatitis.
METHOD
This study used an analytical cross sectional study design to examine the relationship between serum TPO levels and degrees of liver fibrosis in 62 patients with chronic hepatitis from June 2006 to March 2008. Screening of patients was conducted at several hospitals in Medan and Jakarta.
Histopathologic tissue examinations by liver biopsy were done on patients to verify the degree of fibrosis in accordance to Metavir system score in each patient with chronic hepatitis.12,13,14 Blood samplings to establish the levels of serum TPO were accomplished by Quantikine Human TPO immunoassay. We then performed statistical analysis with Spearman’s correlation test to assess the relationship of serum TPO levels and severity degrees of liver damage (fibrosis). Furthermore, the sensitivity and specificity of TPO in diagnosing the degree of liver fibrosis can be determined.15,16
RESULTS
From a number of 62 samples, only 55 patients met the inclusion criteria, which consisted of 22 female and 33 male with an age range of 18-70 years old. A total of 38 patients suffered from hepatitis B, 15 patients from hepatitis C, and 2 patients from non B & non C hepatitis. This study also included 11 people from the normal group and 10 patients with liver cirrhosis.
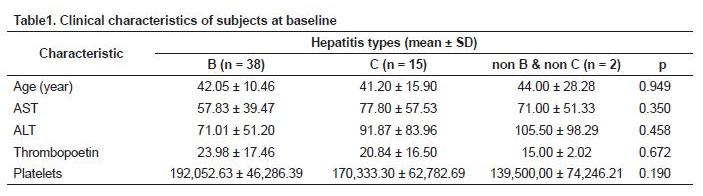
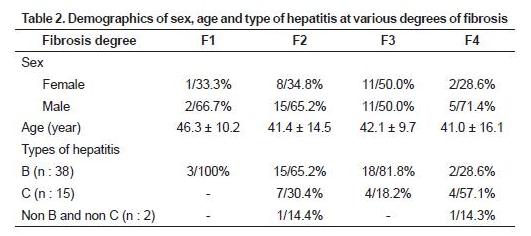
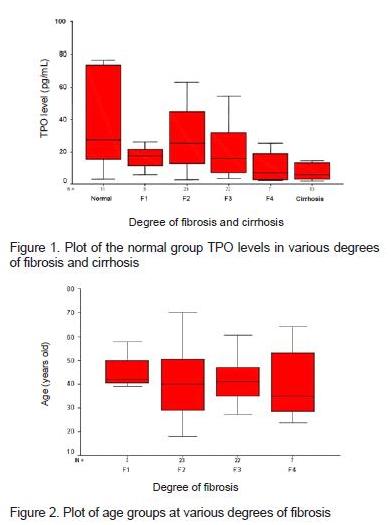
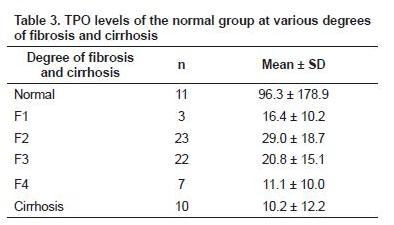
Table 3 shows that the difference in the TPO level started at second-degree fibrosis and higher. The result of different levels testing on the six groups above, with analysis of variance (ANOVA), also showed a significant difference in levels, i.e. p = 0.047. To get the cut off value of TPO levels that provide the highest sensitivity and specificity, receiver operating characteristics (ROC) analysis was done.
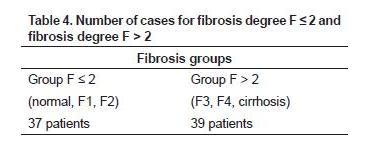
The analysis concluded that there were 37 patients with second-degree fibrosis or less (normal, F1, F2) and 39 patients with higher than second-degree fibrosis (F3, F4 or cirrhosis).
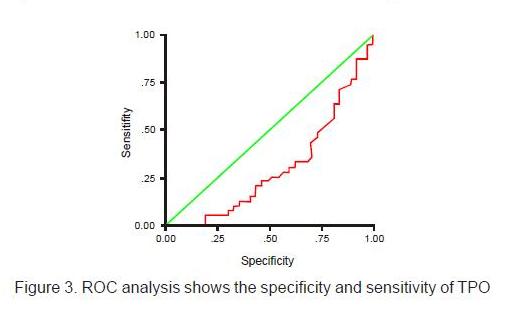
The area under the curve, as big as 0.302, is very significant (p = 0.003), different from 0.5 (95% confidence interval 0.184 – 0.421). By multiplying the sensitivity with the highest specificity, a cut-off 16.01 was obtained. At this value, the specificity and sensitivity of TPO were 64.1% and 70.3% respectively. Chi-square Pearson test results showed a highly significant association between decreased levels of TPO and second-degree fibrosis or higher (p = 0.003).
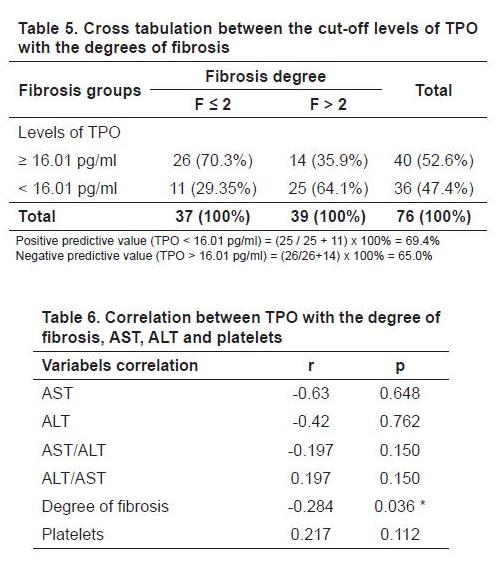
Table 6 shows that the correlations between TPO with AST, ALT, AST/ALT, ALT/AST, and platelets were not significant (p > 0.05), while the correlation of TPO with the degree of fibrosis was significant (p< 0.05). This shows that the smaller TPO level, the greater the degree of fibrosis.
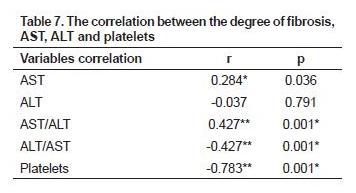
Table 7 shows that the correlation between the degree of fibrosis and AST, and ALT were not significant (p > 0.05), though the correlation coefficient between the degree of fibrosis with AST = 0.284. Meanwhile the degree of fibrosis correlated with the ratio of AST/ALT, ALT/AST and platelets were significant (p < 0.05).
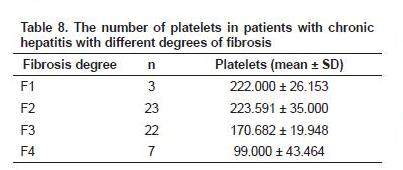
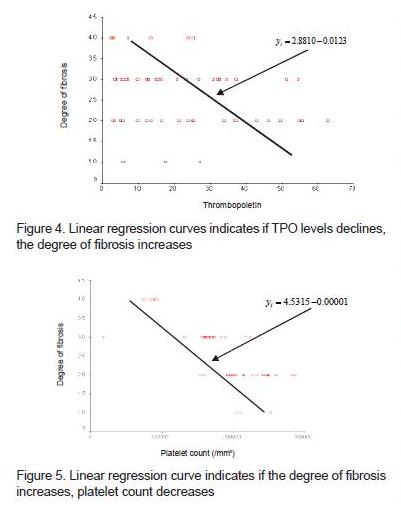
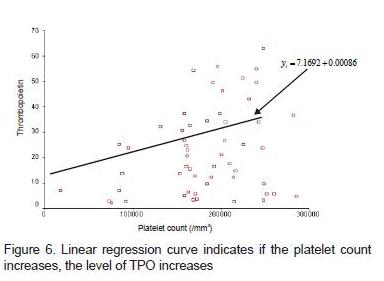
Differences of platelets for each degree of fibrosis were significantly different (p = 0.0001). In the ANOVA test, there were significant differences between the degree of fibrosis and the mean platelet. The differences were the F1 degree of fibrosis compared with F3, F1 with F4, F2 with F3, and F2 with F4. It can be seen in figure 4 that the line formed shows a negative relationship trait; that is when the TPO levels declines, the degree of fibrosis increases. In figure 5, it is known that the line formed shows a negative relationship trait, where if the degree of fibrosis increases, the number of platelets decreases. In figure 6 it is noted that the line that formed showed positive relationship trait, where if the platelet count increases, the TPO level increases.
From the results of Spearman’s correlation test, it was found that levels of TPO have a very significant negative correlation with the degrees of liver fibrosis (r = -0.284; p < 0.05). At the cut-off 16.01 pg/mL, the sensitivity and specificity of TPO in diagnosing the degree of fibrosis greater than F2 (F3 or greater) is obtained, i.e. 64.1% and 70.3% respectively. If the TPO concentration is less than 16.01 pg/mL, it is significantly associated (p = 0.003) with F3, F4 or cirrhosis of the liver. In addition, there were significant differences between the degrees of fibrosis and platelet counts (F1 : 222,000 ± 26,153; F2 : 223,590 ± 35,000; F3 : 170,681 ± 19,948; F4 : 990,000 ± 43,464; < 0.0001). A significant negative correlation between the degrees of fibrosis and platelet levels (r = -0.783; p = 0.001) was also found. Thus, the more severe the degree of fibrosis, the lower the platelet counts.
DISCUSSION
Liver fibrosis results from chronic damage to the liver associated with excessive accumulation of ECM proteins. It can be found in many types of chronic liver diseases. Accumulation of ECM proteins would damage the architecture of the liver with the formation of fibrous connective tissue and the development of nodules. When the nodules had formed, the condition is called cirrhosis. Liver fibrosis is described as a wound healing response to chronic liver injury.8 In chronic liver disease, chronic liver injury occurs, causing decreased production of TPO. TPO levels in patients with chronic hepatitis and cirrhosis of the liver decreased in accordance with the severity of the liver disease. This occurs due to the inadequate TPO production in patients who experience severe necroinflammation activity.17,18,19 In chronic liver disease, hematological disorders in the form of thrombocytopenia is also frequently found but the mechanisms of pathogenesis is still not perfectly known.19
Through this study, it was noted that the development of hepatic fibrosis might cause disruption to the production of TPO and subsequently, cause a reduction in the number of platelets. This is consistent with Afdal et al who reported that the decrease of TPO synthesis correlates with the progression of chronic liver disease.20 In Medan, Ginting had measured the serum TPO levels in patients with liver cirrhosis.21
In this study, the 55 patients who fulfilled the inclusion criteria consisted of 38 patients with hepatitis B, 15 patients with hepatitis C 15 and 2 patients with non B and non C hepatitis. It is visible that in the community the rejection rate to participate in a study was still high compared with the high prevalence of chronic hepatitis in Indonesia. Because biopsy is an invasive method, the measurement of serum TPO levels in determining the severity of liver damage is more acceptable due to its non-invasive methods.
No significant difference in sex, age and type of hepatitis virus between groups of fibrosis was shown in this study. This is in accordance with previous studies because the risk of getting hepatitis can be found in any age group regardless of sex differences (tables 2 and 3).
Some studies on the relationship between TPO levels and degrees of severity of liver disease have been reported and is still controversial. Studies which supports the idea that levels of serum TPO decreases in accordance with the severity degree of liver disease (fibrosis) were reported by Goulis et al, Wien et al, Koruk et al, Adinolfi et al.12,17,18,19 The results of other studies which do not support reduced levels of serum TPO is in accordance with the degree of severity of liver disease (fibrosis) were reported by Freni et al, Schoffski et al, Shi et al.22,23,24
TPO levels will decrease in conformity with increase in the severity of liver damage characterized by the degree of fibrosis through liver biopsy. In this study it is shown that with more severe degree of liver damage serum TPO level will decline progressively, TPO levels in healthy people, F1, F2, F3, F4 and cirrhosis: 96.3 ± 178.9 (normal); 16, 4 ± 10.2 (F1); 29.0 ± 18.7 (F2), 20.8 ± 15.1 (F3); 11.1 ± 10.0 (F4) and 10.2 ± 12.2 (cirrhosis) consecutively (table 3). This is consistent with previous study and further strengthen that TPO is synthesized in the liver. So if there is damage to the liver, the level will decrease further. TPO level also inverses with the degrees of fibrosis.
In figure 1 it was found that serum TPO levels in F1 is lower than in F2 and F3. This is possible because TPO is produced in hepatocytes cells, but the regulation is in the circulation (peripheral). TPO has a receptor on megakaryocytes and platelets. If TPO binds to receptors on the platelets, TPO will be destroyed by platelets (down regulation), whereas when bound to receptors on megakaryocyte, TPO will stimulate megakaryocyte to form platelets.
TPO is a cytokine as well as a hormone, which molecularly its reaction to the receptors of different cells is not equal. This could occur due to different signal transduction depending on its receptors. This condition causes the possibility of lower serum TPO levels in F1 than in the F2 and F3.
Statistically significant difference was seen between TPO levels in F2 and cirrhosis (p = 0.03) whereas the difference between F2 and F4 is on the borderline (p = 0.053). This is probably due to the relatively small number of samples in the group of F4 in this study. Ideally the numbers of samples in each sample population subgroups are the same (homogeneous).
The study involved several national and regional referral center hospitals, where in a relatively long time the number of cases found was still small (55 cases), despite evidence that showed that TPO levels is inversely proportional to the staging of fibrosis. Because of that it is necessary to find limits TPO levels that can be used as a cut off value to determine the degree of chronic hepatitis fibrosis. In this study, with TPO levels 16.01 pg/mL, the sensitivity was 64.1%, specificity 70.3%, positive predictive value 69.4% and negative predictive value 65%. These values were high enough when compared to the gold standard, which has limitations. It was also noted that the cut-off value 16.01 pg/mL can distinguish whether patients has a more severe degree of liver damage or not. If the value of TPO < 16.01 pg/mL, the liver damage is more severe (F3 or greater) and cirrhosis may occur (F4). If levels of TPO > 16.01 pg/mL, then the liver damage is lighter (normal, F1 or F2). From this study, a significant negative correlation between the degrees of fibrosis and platelet was obtained (p < 0.05; r = -0.783) and a positive correlation between the ratio of AST/ALT with the degree of fibrosis (r = 0.427; p = 0.001) was found. Thus, this result is a new finding, that by measuring serum TPO levels we can determine whether a person is suffering from chronic hepatitis, especially with the higher than F2 degree of fibrosis. In previous study, there has not been any that tells us the cut-off levels of TPO in determining chronic hepatitis.
From the results of a study on chronic hepatitis patient groups with F1 to F4 degrees of fibrosis and cirrhosis, a negative correlation to serum TPO levels (r = -0.284; p = 0.036) was found (table 6), which indicates that if the degree of liver fibrosis increases, the levels of serum TPO decreases. This is consistent with a study conducted by Adinolfi et al.12 In this study, TPO levels were found significantly different on the second degree fibrosis (F2) compared with forth degree (F4) with p = 0.001. Kaushansy et al reported that age did not affect the levels of TPO.11 This situation can be explained because TPO is synthesized in the liver and the level will decrease if there is an increasingly severe liver injury. Until now the gold standard in assessing the degree of liver fibrosis is by liver biopsy, which is invasive. It is necessary to determine the degree of liver fibrosis in patients with chronic hepatitis especially B and C viruses, with the aim to initiate, evaluate the treatment and determine the prognosis of the disease.
Although some previous study has been done abroad, the determination of a cut-off value of TPO for its usage in determining the severity degree of liver disease does not exist, even though the determination of a cut-off value can then be used to determine the severity degree of liver disease or in assessing the success of treatment of chronic liver diseases. The study found that by using a cut-off value 16.01 pg/mL we will be able to distinguish whether a patient has a more severe degree of liver damage or not. If the value of TPO < 16.01 pg/mL, it indicates that the liver damage was relatively severe, the patient has third degree of fibrosis (F3) minimum. Meanwhile, when the level of TPO > 16.01 pg/mL, it indicates that the patient is suffering from liver disease with the first (F1) or second (F2) degree of fibrosis or even a non-chronic hepatitis. Ideally this cut-off value should be able to determine the F2 degree because chronic hepatitis caused by hepatitis B or C virus will begin treatment at F2 degree. In this study it cannot be employed because of the small sample size and the inhomogeneous data distribution. However, the cut-off value 16.01 pg/mL can actually be used to evaluate the degree of severity and the therapy of chronic hepatitis because with the cut-off value < 16.01 pg/mL, F3, F4 degrees and cirrhosis can be determined.
TPO is a hormone produced by the liver, which function to stimulate the formation of platelet. This statement was frequently mentioned in previous researches.18,19 However, a significant correlation between the levels of TPO and platelet counts (p > 0.05) was not shown. Platelet levels in patients with chronic hepatitis were inversely proportional to the degree of fibrosis (F1-F4).
The fact is all this time in patients with chronic hepatitis or cirrhosis, decrease in platelets was proportional to the severity of liver damage, especially in patients with hepatitis C, although lower levels of platelets showed no severe thrombocytopenia that causes spontaneous bleeding (platelets < 10,000/mm3) or risk of bleeding with invasive measures (platelet 20,000-50,000/mm3). Decrease in platelet count in patients with chronic hepatitis addresses the need for vigilance for risk of bleeding caused by rupture of varicose veins in liver cirrhosis. In this study a very significant difference between the degree of liver damage and platelet counts (p = 0.0001) was noted.
This study found that serum TPO levels negatively correlated with the degree of severity of liver fibrosis (p = 0.036; r = -0.284) and positively correlated with levels of platelets (p = 0.112; r = 0.217). Thrombocytopenia can occur if the number of platelets in the blood < 100,000/mm3. This is a common complication of chronic liver disease, but the pathogenesis is not clear. It is estimated that the congestion of the spleen is due to portal hypertension (which is the main etiological factor), increased destruction of platelets, decreased production of platelets and anti-platelets antibodies, the occurrence of disseminated intravascular coagulation, translocation of toxin or substances derived from the gastrointestinal tract, and portosystemic shunting.25
Important observation in some previous studies illustrated that TPO plays a major role in regulating platelet production physiologically. TPO levels decreased in patients with chronic hepatitis and cirrhosis. TPO mRNA levels in the liver tissue decreased with progressive liver disease in humans and mice. TPO levels increased significantly after liver transplantation and then perfect resolution of thrombocytopenia occurred after transplantation. All this supports that thrombocytopenia in chronic liver disease is not only due to splenic sequestration, but also because of reduced production of platelets due to decreased synthesis of TPO.15,25-31
Some researchers reported the correlation of peripheral platelet count with the severity degree of fibrosis in patients with chronic hepatitis C. More recently researchers have also reported the same result on people with chronic hepatitis B. Their study of patients with chronic hepatitis B and C demonstrated a decrease in peripheral platelet counts that correlate with liver injury. Peripheral platelet count correlated negatively with the fibrosis score and necroinflammatory activity (NIA). Treatment of hepatitis C virus infection progressed much since the introduction of combination therapy of interferon and ribavirin. Many factors affect the response to treatment including histological stage of disease. Patients with severe fibrosis or cirrhosis at the time of diagnosis failed to give good treatment results and more often end up with advanced-stage liver disease compared with patients without severe fibrosis.15,25,26
Consensus of National Institutes of Health recommends performing a liver biopsy before starting treatment.32 With so many obstacles or difficulties in doing a liver biopsy, many efforts were made to avoid this invasive liver biopsy. A simple non-invasive laboratory method that can predict the degree of fibrosis can be used as an alternative to lessen liver biopsy before physicians provide treatment to patients with chronic hepatitis. Some researchers tried to use aminotransferase ratio, which is sometimes combined with other laboratory parameters to predict severe liver fibrosis or cirrhosis, but the results are still controversial. For aminotransferase itself, its positive predictive value is still quite low. Other researchers estimate that the number of platelets may be associated with fibrosis.
In studies conducted by Pohl et al and Shin et al predicting cirrhosis using the ratio of AST/ALT in evaluating the starting point of patients with hepatitis C virus infection was attempted.33,34 It was reported that the ratio of AST/ALT and platelet count correlated with the degree of fibrosis in patients without history of excessive alcohol drinking. The combination of the ratio of AST/ALT ≥ 1 and platelet count ≤ 150,000/mm3 can detect patients with severe fibrosis (grade 3 and 4) positively with high predictive value (93.1%) and specificity (99.1%).33
In this study, Spearman’s correlation test was also done between the degree of liver fibrosis and the ratio of AST/ALT and results that correlated positive significantly (p = 0.001; r = 0.427) was obtained. If the ratio of AST/ALT is greater, then the degree of liver fibrosis magnifies. The discovery of fibroscan, which is a novel non-invasive imaging to measure the degree of fibrosis, when connected or combined with examination of serum TPO levels produce higher sensitivity and specificity.
In addition, it is found that serum TPO levels negatively correlated with the severity degree of liver fibrosis and positively correlated with levels of platelets. Moreover, a positive correlation between the degree of liver fibrosis with the ratio of AST/ALT was found.
CONCLUSION
A significant negative correlation between serum TPO levels and the degree of liver fibrosis in patients with chronic hepatitis, in which serum TPO levels with the cut-off 16.01 pg/mL can diagnose the F3 degree or greater, was found. A significant negative correlation between the degree of fibrosis and platelet levels was
also noted.
REFERENCES
- Tsukahara A, Sato Y, Yamamoto S, Suzuki S, Nakatsuka H, Watanabe T, et al. Thrombopoietin levels and peripheral platelet counts following living related donor liver transplantation. Hepatogastroenterology 2003;50:227-30.
- Sherlock S, Dooley J. Chronic hepatitis: general features an autoimmune chronic disease. In: Diseases of the Liver and Biliary System. 10th ed. USA: Blackwell Scientific Publ 1997.p.321-32.
- Akbar N. Hepatitis B dan hepatitis C. In: Sulaiman A, Akbar N, Lesmana LA, Noer MS, eds. Buku Ajar Penyakit Hati. 1st ed. Jakarta: FKUI 2007.p.201-8.
- Shearman DJC, Finlayson NDC. Chronic hepatitis in diseases of the gastrointestinal tract and liver. Edinburgh London Melbourne and New York: Living Stone Inc 1982.p.570-80.
- Berenguer M, Wright TL. Viral hepatitis. In: Schiff ER, Sorel. MF, Maddrey IE, eds. Disease of the Liver. Philadelphia 1998.p.1278-323.
- Friedman L. Hepatic fibrosis. In: Schiff’s Diseases of The Liver. 8th ed. Philadelphia: 1982.p.371–82.
- Friedman SC, Runyon BA, Bonis PA. Pathogenesis of hepatic fibrosis. Last Literature Review. Version 16.1:Jan 2008.
- Friedman SL. Liver fibrosis – from bench to bedside. J Hepatol 2003;38:S38-53.
- Huebert RC, Shah VH. Hepatic sinusoidal endothelial cells. In: Dufour JF, Clavien PA, eds. Signaling Pathways in Liver Disease. 2nd ed. New York: Springer 2005.p.53-9.
- Pinzani M, Rombouts K, Colagrande S. Fibrosis in chronic liver diseases: diagnosis and management. J Hepatol 2005;42:S22-36.
- Kaushansky K. Thrombopoetein: the primary regulator of platelet production. Blood 1995;86:419-31.
- Adinolfi LE, Giordano MG, Andreana A, Tripodi MF, Utili R, Cesaro G, et al. Hepatic fibrosis plays a central role in the pathogenesis of thrombocytopenia in patients with chronic viral hepatitis. British J Haematol 2001;113:590–5.
- Hasan I. Biopsi hati. In: Sulaiman A, Akbar N, Lesmana LA, Noer MS, eds. Buku Ajar Ilmu Penyakit Hati. 1st ed. Jakarta: Jayabadi 2007.p.31-6.
- Amirudin R. Fibrosis hati. In: Sulaiman A, Akbar N, Lesmana L A, Noer MS, eds. Buku Ajar Ilmu Penyakit Hati. 1st ed. Jakarta: Jayabadi 2007.p.52-9.
- Afdhal NH, Nunes D. Evaluation of liver fibrosis: a concise review. Am J Gastroenterol 2004;99:1160-74.
- Bataller R, Brenner DA. Liver Fibrosis. J Clin Invest 2005;115:209-18.
- Goulis J, Chau TN, Jordan S, Mehta AB, Watkinson A, Rolles K, et al. Thrombopoietin concentrations are low in patients with cirrhosis and thrombocytopenia and are restored after orthotopic liver transplantation. Gut 1999;44:754-8.
- Peck-Radosavljevic M. Thrombocytopenia in liver disease. Can J Gastroenterol 2000;14:60D-66D.
- Koruk M, Onuk MD, Akçay F, Savas MC. Serum thrombopoietin levels in patients with chronic hepatitis and liver cirrhosis, and its relationship with circulating thrombocyte counts. Hepatogastroenterology 2002;49:1645-8.
- Afdal N, McHutchison J, Brown R, et al. Thrombocytopenia associated with chronic liver disease. J Hepatol 2008;40:1000-7.
- Ginting F. Kadar Trombopoitin Serum Pada Penderita Sirosis Hati. Thesis Program Pendidikan Dokter Spesialis Ilmu Penyakit Dalam, Universitas Sumatera Utara 2005.
- Freni MA, Spadaro A, Ajello A, Barbaro E, Scaffidi M, Alessi N, et al. Serum thrombopoietin in chronic liver disease: relation to severity of the disease and spleen size. Hepatogastroenterology 2002;49:1382-5.
- Schöffski P, Tacke F, Trautwein C, Martin MU, Caselitz M, Hecker H, et al. Thrombopoietin serum levels are elevated in patients with hepatitis B/C infection compared to other causes of chronic liver disease. Liver 2002;22:114-20.
- Shi Y, Hou M. Plasma thrombopoietin level and its influence on megakaryocytopoiesis in end-stage liver cirrhosis and uremia patients. Zhongguo Shi Yan Xue Ye Xue Za Zhi 2002;10:590-2.
- Karasu Z, Tekin F, Ersoz G, Gunsar F, Batur Y, Ilter T, et al. Liver fibrosis is associated with decreased peripheral platelet count in patients with chronic hepatitis B and C. Dig Dis Sci 2007;52:1535-9.
- Watanabe M, Murata S, Hashimoto I, Nakano Y, Ikeda O, Aoyagi Y, et al. Platelets contribute to the reduction of liver fibrosis in mice. J Gastroenterol Hepatol 2009;24:78-89.
- Ono E, Shiratori Y, Okudaira T, Imamura M, Teratani T, Kanai F, et al. Platelet count reflects stage of chronic hepatitis C. Hepatol Res 1999;15:192-200.
- Witters P, Freson K, Verslype C, Peerlinck K, Hoylaerts M, Nevens F, et al. Blood platelet number and function in chronic liver disease and cirrhosis. Aliment Pharmacol Ther 2008;27:1017-29.
- Chu CW, Hwang SJ, Lu RH, Lai CR, Luo JC, Wang YJ, et al. Clinical significance of the changes of platelet counts and serum thrombopoietin levels in chronic hepatitis C patients treated with different doses of consensus interferon. Hepatol Res 2002;24:236-44.
- Poordad F. Review article: thrombocytopenia in chronic liver disease. Aliment Pharmacol Ther 2007;26:5-11.
- Wang CS, Yao WJ, Wang ST, Chang TT, Chou P. Strong association of hepatitis C virus (HCV) infection and thrombocytopenia: implications from a survey of a community with hyperendemic HCV infection. Clin Infect Dis 2004;39:790-6.
- Belongia EA, Costa J, Gareen IF, Grem JL, Inadomi JM, Kern ER, et al. National Institutes of Health Consensus Development Conference Statement: management of hepatitis B. Ann Intern Med 2009;150:104-10.
- Pohl A, Behling C, Oliver D, Kilani M, Monson P, Hassanein T. Serum aminotransferase levels and platelet counts as predictors of degree of fibrosis in chronic hepatitis C virus infection Am J Gastroenterol 2001;96:3142-6.
- Shin WG, Park SH, Jang MK, Hahn TH, Kim JB, Lee MS. Aspartate aminotransferase to platelet ratio index (APRI) can predict liver fibrosis in chronic hepatitis B. Dig Liver Dis 2008;40:267-74.
Correspondence:
Juwita Sembiring
Department of Internal Medicine
Adam Malik Hospital
Jl. Bunga Lau No. 17 Medan 20136 Indonesia
Phone: +62-61-8365741 Fax: +62-61-8363009
E-mail:wita_sm@yahoo.com
———- End