")
Source : Acta Med Indonesia-Indonesia Journal International Medicine, Vol 42, Number 3, July 2010
Written by : Ni Made Renny A. Rena, I Dewa Nyoman Wibawa
Department of Internal Medicine, Faculty of Medicine, University of Udayana-Sanglah Hospital. Jl. PB. Sudirman, Denpasar Bali, Indonesia.
Correspondence mail to: pipfkui@yahoo.com
ABSTRACT
Albumin infusions have been used for many years in the management of patients with decompensated cirrhosis in an attempt to reduce the formation of ascites, to improve circulatory and renal function, or in SBP patients. While some of these indications for albumin infusions are supported by the results of randomised studies, others are based on clinical experience and have not been proved in prospective investigations. Therefore, the use of albumin infusions in patients with cirrhosis is still controversial. However, despite the controversies, the use of albumin at least has been proven to be safe. Some guidelines recommended the use of albumin infusion in decompensated cirrhosis with spontaneous bacterial peritonitis, hepatorenal syndrome, large volume parecentesis and decompensated cirrhosis with complications.
Key words : Albumin, liver cirrhotic.
INTRODUCTION
Liver cirrhosis, especially in the presence of decompensation, is characterized by significant hemodynamic changes. These changes consist of systemic arterial vasodilatation, and effective arterial underfilling, which stimulate the renin aldosteron angiotensin system and associated with renal retention of sodium and water, and ascites is one of their clinical manifestations. In addition, patients with liver cirrhosis are susceptible to sepsis, especially bacterial infections. Once infection develops, renal failure, shock and encephalopathy can follow, all of which adversely affect survival and increase mortality.
Albumin is the most abundant protein in the circulation, which has multiple function that can be used in cirrhotic patients with those complications mention above. The main physiologic function of albumin is to maintain intravascular volume and colloid osmotic pressure. The other physiologic functions of albumin include ligand binding and transport of various molecules, such as hormones, lipid and drugs. In addition to having antioxidant and antiinflammatory actions, and stabilizing effect on the endothelium.1-4
The use of albumin for many of these indications is controversial, some studies support it based on the decreasing of mortality rate of these patients. The other indication for albumin use in cirrhotic patients is extracorporeal albumin dialysis, which has shown promise for the treatment of hepatic encephalopathy. Some studies debate this mostly because of the cost of albumin infusions, the lack of clear-cut benefits for survival, and for fear of transmitting unknown viruses such as hepatitis B, hepatitis C and also HIV adding to the controversy, allthough some studies say it is safe.1,5 Finally, it still requires further discussion, studies and evidences for administration albumin in cirrhotic patients.
ALBUMIN
In healthy individuals, albumin is the most abundant plasma protein, accounting for 55-60% of the measured serum protein. It consists of a single polypeptide chain of 585 amino acids with a molecular weight of 66 500 Da. The mature, circulating molecule is arranged in a series of α-helices, folded and held by 17 disulphide bridges.2
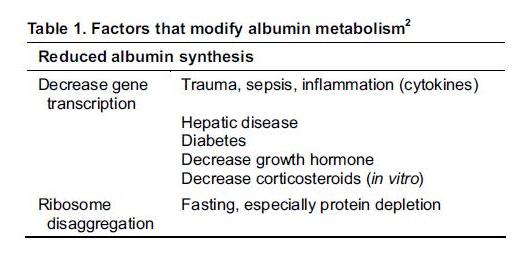
The serum albumin concentration is a function of its rate of synthesis and degradation and its distribution. Albumin synthesis takes place only in the liver, with the rate of synthesis 197 mg/kg body weight/day or about 12-25 g of albumin per day. Albumin is not stored by the liver but secreted into the portal circulation as soon as it is manufactured. Physiologically, the liver can increase albumin synthesis to only 2-2.7 times normal. Some factors required for the albumin synthesis are suitable nutritional, hormonal and osmotic environment. The colloid osmotic pressure (COP) of the intertitial fluid bathing the hepatocyte is the most regulator of albumin synthesis. Some factors to modify albumin metabolism are on Table 1.1,2,6
Each day, the total body albumin pool measure about 3.5-5.0 g/kg body weight or about 250-300 g for a healthy 70 kg adult. Distribution of albumin to the intravascular compartment is about 42%, and the rest being in extravascular compartment. Most of albumin in extravascular space is recovered back into the circulation by lymphatic drainage. Albumin lost into the intestinal tract about 1 g, and only few grams (about 10-20 mg/day) pass through the kidney as urinary loss.2
Albumin degradation in a 70 kg adult every day is around 14 g or 5% of daily whole body protein turn over. Albumin is broken down mostly in muscle and skin (40-60%) and other organs in the body such as liver, kidney and gastrointestinal tract.2
Albumin being extensively studied and well established has numerous functions used in many clinical situations, including:1,2,7
- Maintaining colloidal osmotic pressure
- Ligand binding of numerous endogenous and exogenous compounds
- Effective as plasma buffer
- Antioxidant effects
- Endothelial stabilization
- Anti coagulant
HYPOALBUMINEMIA IN LIVER CIRRHOTIC PATIENTS
Liver cirrhotic is a protein catabolic disease, which at the advanced stages is usually associated with loss of lean body mass and decreased albumin concentration. Moriwaki, et al in 2001 found that 40% with protein malnutrition, 10% with energy malnutrition, 30% with protein-energy malnutrition and 20% with normal nutritional state. Other study by Merli, et al in 1996 found malnutrition is strongly associated with the deterioration of liver function, and considered as a dependent risk factor for mortality in cirrhotic patients.4,8
Hypoalbuminemia in liver cirrhotic patients is due to:4,9
- Decrease of albumin synthesis in the liver
- Increase of albumin catabolism
- Vascular leakage due to increase of membarane permeability such as ascites and oedem.
- Capillary leakage, such as sepsis and shock.
ALBUMIN INFUSION IN LIVER CIRRHOTIC PATIENTS
The indication of giving albumin in liver cirrhotic patients are:
Spontaneous Bacterial Peritonitis (SBP)
Spontaneous bacterial peritonitis (SBP) is a common and often fatal complication of cirrhosis with high mortality rate. Mortality in patients with SBP is caused by gastrointestinal bleeding, liver failure and around 30-40% fall into Hepato Renal Syndrome.1,4
In patients with SBP, there is a risk that their systemic hemodynamic parameters can deteriorate, with further arterial and splanchnic vasodilatation. These patients are, therefore, at high risk of developing renal insufficiency. Peritonitis and the release of high level of vasoactive cytokines in sepsis are considered as the patophysiological explanation for the association between SBP and renal insufficiency. Vasoactive cytokine worsens the arterial vasodilatation and results in secondary activation of neurohormonal system. Therefore, the use of albumin is to maintain intravascular volume and to repair renal perfussion.1,3,4
Pau Sort, et al. at 1999, have done a randomized study in 7 hospitals in Spain and found that the administration of albumin prevents renal impairment and reduces mortality in patients with cirrhosis and spontaneous bacterial peritonitis. The incidence of renal impairment was significantly lower among patients treated with cefotaxime and albumin than among patients treated with cefotaxime alone, which is 29%, by contrast, the group treated with cefotaxime and albumin was only 10%. However, this study received many criticisms because of unblind randomization study and without the insertion of CVP lines in all the patients in order to know the relationship with the disorder of renal function. Besides, this study also didn’t make comparison between albumin and others plasma expanders.10,11
Study in 2005 by Fernandez, et al. compared the role of albumin and hydroxyethyl starch (HES) to prevent renal failure in SBP patients, found that albumin has it’s superiority than HES.12 Another study compared albumin, crystalloid fluid and artificial colloid give the same result.13 Although albumin has a significant role in SBP patients with severe disturbance of liver and renal function, but it’s use is still debated because of the high cost.3,14,15 Other opinion says patients with sepsis have an increase vascular permeability, therefore albumin as well as other molecule may became far less efficient in maintaining effective plasma volume for longer period because of rapid leakage from circulation. It still need to do further study.3 The third phase of study has been done until now about the role of human albumin in cirrhotic patients with infection other than SBP. This study was held in February 2008.16
The other practice guidelines to follow are regarding to recommendation of American Association for the Study of Liver Diseases (AASLD) and Indonesian Association for the Study of the Liver. It suggested that patient clinical suspected of SBP should receive albumin 1,5 g/kg body weight within 6 hours of detection and should be given lower dose 1 g/kg body weight on day 3.4,14,17
Hepato Renal Syndrome
Hepatorenal syndrome (HRS) is a dreaded complication of advanced cirrhosis. HRS is defined as the development of renal failure in patients with advanced liver failure (acute or chronic) in the absence of any identifiable causes of renal pathology. Untreated type 1 HRS carries a grim prognosis and high mortality as 80% in second week and only 10% of patients survived more than 3 months. The prognosis can be assessed by CHILD-PUGH and MELD (Model of End-Stage Liver Disease) as an independent predictor of death which is with score of 20 or more being only 1 month compared with 8 months in those with a MELD score <20. By contrast, patients with type 2 HRS have a much better median survival, approximately 6 months.18
The hallmark of HRS is renal hypoperfusion, which is caused by reduction renal blood flow result from condition of systemic arterial vasoconstriction. The effective arterial underfilling is caused by splanchnic vasodilatation. Renal vasoconstriction occurs as the result of both active renal vasoconstriction and reducing systemic vasodilator factor such as prostaglandine, Nitric Oxyde (NO) and natriuretic peptide as the compensated action due to systemic arterial vasodilatation.4,18
The goal of treatment in SHR is to reduce systemic vasodilatation and increase renal blood flow. Besides renal transplantation and hemodialysis, pharmacotherapies have been recommended in systemic vasoconstrictors as vasopressin analogs or α-adrenergic agonists. The use of albumin to improve arterial underfilling is also recommended in combination with vasoconstrictors, ocreotide or midodrine. Some authors believe that albumin can improve the efficacy of vasoconstrictors therapy.
Angeli et al. in 2003 reported the superiority of administration dopamin together with albumin at non intensive ward in type 1 HRS.19 Another pilot study done by Duvoux, et al. using norepinephrine plus albumin, reports 83% success in reversing type 1 HRS. American Association for the Study of Liver Diseases
(AASLD) recommended that albumin infusion plus administration of vasoactive drugs such as ocreotide and midodrine should be considered in the treatment of type 1 HRS (level II-1). Indonesian Association for the Study of the Liver also recommended that albumin infusion given to prevent HRS in SBP patients combined with cefotaxime can decrease mortality and frequency of HRS. Other study shows it can improve renal function to 60-70%. The dose given is 1 g/kg intravenously in day 1 and followed by 20-40 g/day for 5-15 days or stopped when CVP >18 cm H2O. However, for the preventive dose is 1,5 g/kg body weight in day 1 and 1 gram / kg body weight in the next 48 hours.3,4,14,17,18
A prospective, randomized, controlled study shows that Molecular Adsorbent Resirculating System (MARS), an extracorporeal albumin dialysis, can improved clinical and biochemical parameters in type 1 HRS patients. The advantage of using MARS in HRS relies on the assumption that removing albumin-bound toxins which have a detrimental effect on hepatocytes and other organs, including the kidney, will stabilize liver function and improve other end organ damage.18
Moreau et al. in 2002 doing the largest retrospective study on the use of terlipressin for HRS did not find any difference in patient outcomes irrespective of whether they received albumin infusions as well as terlipressin. However, Uriz et al. in 2000 found that terlipressin combined with albumin was effective for type 1 HRS. Other study found one thirds patients with ischemia as side effect from using ornipressin and albumin.1,13,16-18
Plasma Expansion in Large Volume Paracentesis
The circulatory disturbances seen in advanced cirrhosis lead to the development of ascites, which can become refractory to diet and medical therapy.
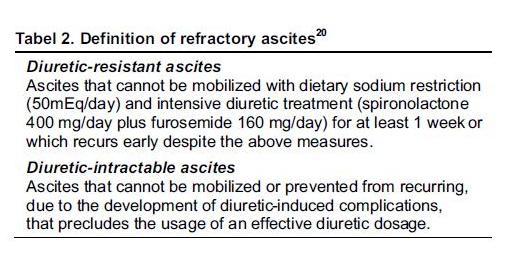
Approximately 10-20% of patients with ascites have adequate natriuresis and clinical response to dietary sodium restriction alone, and the majority of the remaining patients respond to diuretic therapy. However, around 10% of patients do not respond to the above measures, or develop complications to diuretic therapy, and these patients are classified as having refractory ascites. Prognosis for this subgroup of patients is poor, with a 50% 1-year mortality. The International Ascites Club recently redefined refractory ascites.20
One of the management of refractory ascites is Large Volume Paracentesis (LVP). Some studies concluded that serial therapeutic paracentesis can be performed safely and effectively with volume less than 5 litres.17,20-22 Circulatory dysfunction can develop after large-volume paracentesis. This is caused by exaggerated systemic arterial vasodilatation, effective intravascular volume depletion, and elevated renin and aldosterone levels. Clinically it’s recognized as renal impairment and electrolyte imbalance, particularly hyponatremia.1
Albumin infusion seems to be the most appropriate way to prevent this complication of paracentesis. The argument against albumin infusion in conjunction with paracentesis use is further fuelled by the finding that a 5l paracentesis without albumin infusion was not associated with any changes in central blood volume, serum sodium levels or renal function. However some consensus still recommended albumin infusion in LVP.1,23-27
American Association for the Study of Liver diseases (AASLD) recommended that albumin infusion should be given with dose 6-8 g/1 litre ascites fluid removed for paracentesis volumes of greater than 5-6 litres. Fifty percents should be given in the first 1 hour (maximum 170 mL/hr) and the remain in the next 6 hours.14,15
The uses of albumin led to studies investigating substitute fluid for albumin that can prevent circulatory failure after paracentesis. It’s found mannitol has the same effectivity as albumin, but not others plasma expanders like dextran and polygelyne. Hydroxyethyl starch (HES) is still controversy, it concluded there the use was no significantly differences than albumin. It can be tolerated by liver cirrhotic patients, but it still need further investigation about lower weight loss compare to albumin.28-31
Albumin Level <2.5 g/dL in Liver Cirrhotic Patients with Complications
Some complications can occur in liver cirrhotic patients, the low level of albumin leads them into worst condition. Therefore, Indonesian Association for the Study of the Liver in 2003 suggest albumin infusion for those conditions. The dose is different albumin level in every kg body weight.4
Other complications such as electrolyte abnormalities, especially hyponatremia and hyperkalemia, are common in patients with advanced cirrhosis. These abnormalities can occur spontaneously, or more often follow the use of diuretics. Hyponatremia is usually the result of overactivity of vasopressin, in response to a reduction in the effective arterial blood volume Diuretic-induced electrolyte abnormalities and blood-volume contraction can also lead to the development of hepatic encephalopathy in patients with cirrhosis. In a study conducted in cirrhotic patients with diuretic-induced hepatic encephalopathy by Jalan R et al., showed infusion of a 4.5% albumin solution was comparably effective to infusion of a colloid solution in relation to increasing plasma volume. Both treatments caused similar reductions in plasma ammonia concentrations, and increased in urinary ammonia excretion. The improvement of hepatic encephalopathy grade, although it was only sustained at 72 h in the group who received albumin infusions, and was associated with a reduction in plasma malondialdehyde, which suggested a reduction in oxidative stress.7
As the use of albumin in liver cirrhotic patients is still controversial, not only because of lack of clear cut benefits for survival, but also because of the high cost of albumin infusion. Therefore, many studies done to compare effectivity between albumin and other fluids in SBP patients and ascites patients whose done LVP as shown in Table 3.

The debate about the use of albumin in the critically ill patients has been stimulated by the publication of a meta-analysis which reviewed 32 randomized controlled trials published between 1975 and 1998, in which albumin was used in treatment of hypovolemic, burnt or hypoalbuminaemic patients. The data suggested that the use of albumin in these groups resulted in six additional deaths per 100 patients. The controversy seems to have centred on the validity of the conclusions drawn from such a heterogenous group of studies, samples of the studies were small, and there were few deaths. Some of the responses suggested that capillary leakage may explain the increased mortality, and presented data showing that albumin leakage was greater in critically ill patients than in patients after major surgery. Thus, infusion of albumin in the critically ill patients would not increase the intravascular albumin concentration, and would exacerbate interstitial oedema.2, 32
Further explanations of why albumin might not work is because of the beneficial effects of albumin in the circulation, such as the binding of toxins, heavy metals and drugs, are detrimental outside of the circulation, given the increase in capillary permeability during critical illness. There may also be the adverse immunological effects of albumin transfusion that could explain the increase in mortality suggested by this meta analysis.2,32
Arroyo and Gines in 2000 wrote a controversial article about whether there is still a need for albumin infusions to treat patients with liver disease. There is a strong body of evidence indicating that renal functional abnormalities and ascites formation in cirrhosis are the final consequence of circulatory dysfunction, characterized by marked splanchnic arterial vasodilatation causing a reduction in effective arterial blood volume and homeostatic activation of vasoconstrictor and antinatriuretic mechanisms.In contrast, there is no evidence to support a role for reduced vascular oncotic pressure due to hypoalbuminaemia in the pathogenesis of ascites.33
Saline Versus Albumin Evaluation (SAFE) study, a randomized clinical trial in Australia and New Zealand included a heterogeneous population of nearly 7000 critically ill patients requiring intravascular fluid resuscitation. The Australian and New Zealand Intensive Care Society Clinical Trials Group set out to determine the safety of fluid resuscitation with 0.9% normal saline versus 4% human albumin on a number of patient outcomes. There were no significant differences between the groups with respect to 28-day mortality, incidence of organ failure, intensive care unit or hospital length of stay, or duration of mechanical ventilation or renal replacement therapy.34
Indonesian Association for the Study of the Liver suggested that infusion of albumin 20% with maximum rate is 1 mL/minute, and for albumin 5% is 2-4 mL/minute. Some complications can occur after giving albumin infusion such as heart decompensated, lung oedema, increasing of risk of bleeding like the rupture of esophageal variceal, drugs/metals/hormones accumulation in intestitial space, increasing of nitrogen bodies, and also some studies found viral transmission after albumin infusion.4 It’s important to monitor hemodynamic status including vital sign, coagulation (Prothrombin Time and Activated Partial Thromboplastin Time), renal function test and level of albumin serum after transfusion.4
CONCLUSION
Liver cirrhosis, especially in the presence of decompensation, is characterized by significant hemodynamic changes. These changes consist of systemic arterial vasodilatation, and effective arterial underfilling associated with renal retention of sodium and water which is shown as ascites, hepato renal syndrome, and spontaneous bacterial peritonitis. Albumin, with its multiple physiological effects of volume expansion, anti oxidation and endothelial protection, would seem to be the ideal treatment solution for patients with cirrhosis, especially those with complications. The use of albumin in patients with cirrhosis is controversial; there is evidence to support its use in the management of complications of cirrhosis, but there are also arguments against its use in cirrhosis, especially since albumin infusions are costly and survival has not been shown to be improved with this treatment.
Despite this controversies, safety of the use of albumin at least has been proven. Some guidelines recommended by American Association for the Study of Liver Diseases (AASLD) and Indonesian Association for the Study of the Liver suggested the use of albumin infusion in decompensated cirrhosis with spontaneous bacterial peritonitis, hepato renal syndrome, large volume parecentesis and cirrhosis with complication. Future efforts still need to define the
other indications for albumin use, dose of albumin required and predictors of response, so that patients gain the maximum benefit from its administration.
REFERENCES
- Wong Florence. Drug Insight : the role of albumin in the management of chronic liver disease. Nature Clinical Practice Gastroenterol & Hepatol. 2007;4(1):43-51.
- Nicholson JP, Wolmarans MR, Park GR. The role of albumin in critical illness. Br J Anaesth. 2000;85:599-610.
- Avidan B. The use of albumin in all patients with decompensated cirrhosis is not justified. IMAJ. 2005;7:118-20.
- Perhimpunan Peneliti Hati Indonesia. Pemberian albumin pada sirosis hati. Konsensus PPHI-FKUI. Jakarta: Balai Penerbit FKUI; 2003. p. 1-92.
- Matejtschuk P, Dash CH, Gascoigne EW. Production of human albumin solution: A continually developing colloid. Br J Anaesth. 2000:85:887-95.
- Peters T, Jr. All about albumin. Indiana: Academic Pr Inc; 1996. p. 188-250.
- Jalan R, Kapoor D. Reversal of diuretic-induced hepatic encephalopathy with infusion of albumin but not colloid. Clin Sci. 2004;106:47-474.
- Tessari P, Barazzoni R, Kiwanuka E, Davanzo G, Pergola GD, Orlando M, et al. Impairment of albumin and whole body postprandial protein synthesis in compensated liver cirrhosis. Am J Physiol Endocrinol Metab. 2002;282:304-11.
- Reichen J. The role of the sinusoidal endothelium in liver function. News Physiol Sci. 1999;14:117-21.
- Sort P, Navasa M, Arroyo V, Aldeguer X, Planas R, Albor LR, et al. Effect of intravenous albumin on renal impairment and mortality in patients with cirrhosis and spontaneous bacterial peritonitis. N Engl J Med. 1999;341:403-9.
- Michael J. Albumin in spontaneous bacterial peritonitis. N Engl J Med. 1999;341:403-9.
- Fernandez J et al. Randomized unblinded pilot study comparing albumin versus hydroxyethyl starch in spontaneous bacterial peritonitis. Hepatol. 2005;42:627-34.
- Haynes GR, Navickis RJ, Wilkes MM. Albumin administration – what is the evidence of clinical benefit? A systematic review of randomized controlled trials. January 2003. Available at : www.mwilkws@hygeiaassociates.com. Last update January 2003.
- Runyon BA. AASLD Practice Guidelines. Management of adult patients with ascites due to cirrhosis. Hepatol. 1998;27:264- 72.
- Khalid SK, Garcia-Tsao G. Management of the decompensated cirrhotic patient with HCV. The HCV advocate medical writer’s circle. 2003;1:4.
- Gines P. Albumin administration in patients with cirrhosis and infections unrelated to spontaneous bacterial peritonitis. Available at: www.ClinicalTrials.gov. Last update 10 April 2007.
- Gines P, Cardenas A, Arroyo V, Rodes J. Management of cirrhosis and ascites. N Eng J Med. 2004;350:1646-54.
- Wadei HM, Mai LM, Ahsan N, Gonwa TA. In depth review hepatorenal syndrome: Patophysiology and management. Clin J Am Soc Nephrol. 2006;1:1066-79.
- Angeli P. Prognosis of hepatorenal syndrome-has it changed with current practice? Alimentary Pharmacol & Therapeutics Suppl. 2004;3:44-6.
- Suzuki H, Stanley AJ. Current management and novel therapeutic strategies for refractory ascites and hepatorenal syndrome. QJ Med. 2001;94:293-300.
- Krige J, Beckingham IJ. ABC of disease of liver, pancreas, and biliary system. Portal hypertension-2. Ascites, encephalopathy, and other conditions. BMJ. 2001;322:416-8.
- Straus, Gines A, Fernandez-Esparrach G, Monescillo A, et al. Ascites-albumin prevents postparacentesis circulatory dysfunction in cirrhotics. Gastroenterol. 1996;111:1002-10.
- Garcia-Compean D, Zacarias Villarreal J, Bahena Cuevas H, Garcia Cantu DA, Estrella M, Garza Tamez E, Valadez Castillo R, Barragan RF. Total therapeutic paracentesis (TTP) with and without intravenous albumin in the treatment of cirrhotic tense ascites: a randomized controlled trial. Liver. 1993;13(5): pp.233-8.
- Luca A, Garcia-Pagan JC, Bosch J, Feu F, Jimenez W, Gines A, Fernandez M, Escorsell A, Arroyo V, Rodes J. Beneficial effects of intravenous albumin infusion on the hemodynamic and humoral changes after total paracentesis. Hepatol. 1995;22(3):753-8.
- Sola-Vera J, Minana J, Ricart E, Planella M, Gonzalez B, Torras X, Rodriguez J, Such J, Pascual S, Soriano G, Perez-Mateo M, Guarner C. Randomized trial comparing albumin and saline in the prevention of paracentesis-induced circulatory dysfunction in cirrhotic patients with ascites. Hepatol. 2003; 37(5):1147-53.
- Gines P, Tito L, Arroyo V, Planas R, Panes J, Viver J, Torres M, Humbert P, Rimola A, Llach J, et al. Randomized comparative study of therapeutic paracentesis with and without intravenous albumin in cirrhosis. Gastroenterol. 1988;94(6):1493-502.
- Jiang Z, Chengying Y, Dajun W, Xingwu L. Mannitolum infusion on cirrhotic patients with tense ascites treated by paracentesis. Chin Med J. 2000:113(1):27-30.
- Altman C, Bernard B, Roulot D, Vitte RL, Ink O. Randomized comparative multicenter study of hydroxyethyl starch versus albumin as a plasma expander in cirrhotic patients with tense ascites treated with paracentesis. Eur J Gastroenterol Hepatol. 1998;10(1):5-10.
- Allison SP, Lobo DN. Debate: Albumin administration should not be avoided. Crit Care. 2000;4:147-50.
- Vincent JL. Fluid management: the pharmacoeconomic dimension. Crit Care. 2000;4(2):S33-S5.
- Chalasani N, et al. Effects of albumin/furosemide mixtures on responses to furosemide in hypoalbuminemic patients. J Am Soc Nephrol. 2001;12:1010-6.
- Cochrane Injuries Group Albumin Reviewers. Human albumin administration in critically ill patients: systemic review of randomised controlled trials. British Med J. 998;317;235-40.
- Gines P, Arroyo V. Is there still a need for albumin infusions to treat patients with liver disease? Gut. 2000;46;588-90.
- Fan E, Stewart TE. Commentary. Albumin in critical ill: SAFE,but worth its salt? Crit Care. 2004;8;297-9.
——- End